1. Introduction
The hoof capsule is comprised of the hoof wall, sole,
frog, and bulbs of the heels, which, through the
unique continuous bond between its components,
form a casing on the ground surface of the limb that
affords protection to the soft tissue and osseous
structures enclosed within the capsule.
1 The hoof
wall is a viscoelastic structure that has the ability to
deform under load and then return to its original
shape when the weight is removed. It is well accepted
that abnormal weight distribution on the foot
or disproportionate forces placed on a section of the
hoof will, over time, cause it to assume an abnormal
shape.
1-4 These abnormal stresses within the foot
will also predispose the foot to injury or disease.
Increased stress or weight-bearing placed on a section
of the hoof capsule may originate from a single
source or it may be from multiple contributing factors
such as abnormal limb conformation, strike pattern,
amount of work, type of footing, and
inappropriate farrier practices. Excess stress
placed on one section of the hoof capsule can manifest
itself in a variety of ways, such as compressed
growth rings, flares or under-running of the hoof
wall, dorsal migration of the heels, and either focal
or diffuse displacement of the coronary band.6,7
Distortion of the hoof capsule of the forelimbs appears
to be related to limb alignment and load,
whereas deformation in the hind feet appears to be
different and related to propulsion. Because the
hoof capsule distortion of the forelimbs is commonly
associated with lameness and various disease processes,
only the forelimbs will be considered in this
report. Because the "normal" foot has never been
defined, each view will begin with what is perceived
to be an ideal, good, or healthy foot.
1,8 Palpation of
the hoof capsule often complements the visual examination,
and the areas where palpation is relevant
will be included. The goal of evaluating the
hoof capsule is to identify deformation and changes
in growth pattern that indicate abnormal distribution
of forces (stresses) on the foot. Because hoof
capsule distortion and abnormal loading usually accompany
lameness, farriery will form part of or
sometimes the entire treatment. Farriery is used
to help redistribute the load and help improve or
resolve the hoof capsule deformation.
2. Mechanism of Distortion
Evaluation of the hoof capsule morphology will indicate
where the hoof wall is unduly stressed; however,
the evaluation must be coupled with an
understanding of the abnormal distribution of forces
that lead to hoof capsule deformation. Understanding
the biomechanical forces leading to hoof
capsule distortions is also helpful for the clinician in
applying the appropriate farriery to modify these
stresses. There are many excellent reviews of basic biomechanics of the hoof in the veterinary literature.
1-5 Increased load or weight-bearing by a portion
of the wall has three consequences: (1) it may
cause deviation of the wall outward (flares) or inward
(under-running) from its normal position; (2) it
may cause the wall to move proximally; or (3) it may
decrease hoof wall growth. A reduction in load or
weight-bearing generally has the opposite effect.
Briefly, in the standing horse, the weight of the
horse borne by the limb is supported by the ground,
which opposes the weight with an equal and opposite
force. The force exerted on the foot by the
ground is termed the ground reaction force. The
term center of pressure (COP) is the point on the
ground surface of the foot through which the ground
reaction force acts on the foot. The center of pressure
varies among horses but is approximately located
in the center of the solar surface of the foot in
the standing horse. However, when the horse is
moving, the location of the COP changes dynamically.
The position of the COP at any point in the
stride determines the distribution of forces between
the medial and lateral and the dorsal palmar aspects
of the foot. When the center of pressure is
moved to one side of the foot, that side of the foot will
be subject to increased forces. If the COP is moved
in a palmar direction, the weight-bearing or load on
the palmar hoof wall is increased. Relating this to
hoof capsule distortions, if the COP is located more
medially, over time, a medial hoof wall flare (bending)
and a lateral under-running will develop. Or,
if the COP is located more dorsally because of increased
tension in the deep digital flexor tendon, the
hoof capsule will develop a higher heel with a flare
in the dorsal hoof wall. Farriery is used to change
the location of the center of pressure (to some extent)
and change the distribution of forces on the ground
surface of the foot.
3. Limb Conformation
When evaluating hoof capsule deformation, limb
conformation should be considered. Abnormal limb
conformation affects the landing pattern and stance
phase of the stride. Few horses have ideal limb
conformation, and any change in conformation is
going to change the distribution of forces within the
hoof capsule, leading to deformation. In the frontal
plane, the forelimbs should be of equal length and
size and bear equal weight. A line dropped from
the scapulohumeral joint to the ground should bisect
the limb. Certain types of abnormal limb conformation
have been described.9 In the frontal plane,
abnormal conformation is described as valgus (the
limb's segment distal to the affected joint will deviate
laterally) or varus (the distal segment of the limb
will deviate medially). The joint most often affected
is the carpus, and, to a lesser degree, the
metacarpalphalangeal joint. Here, there will be excess
load placed on the hoof opposite the direction of
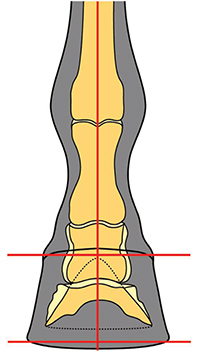
the deviation. If a line dropped from the metacarpalphalangeal
joint through the digit to the ground does not bisect the hoof capsule, the foot is considered
offset to one side (usually laterally) and therefore
increased load is placed on the opposite side of
the foot (Fig. 1).
 |
|
Fig. 1. Distal phalanx within hoof capsule will be offset laterally.
Coronary band will be displaced proximally on media quarter/
heel. |
In the transverse plane, conformation
abnormalities are characterized by axial rotations
of the limb or its segments, either laterally or
medially. For example, a horse with a narrow
chest and a lateral axial rotation will land on the
lateral side of the hoof and then load the medial side
resulting in proximal displacement of the quarter
/heel on the medial side and causing the hoof deformation
termed "sheared heels"10,11 (Fig. 2). A limb
with a medial (inward) rotation of the digit relative
to the third metacarpal bone (toed-in) will develop a
hoof with a diagonal asymmetry, with a narrow lateral
toe and medial heel and a wide medial toe and lateral heel. The altered distribution of forces leading
to hoof capsule deformations follow a logical
pattern in which the overloaded sections of the hoof
are less developed and the under-loaded sections are
overdeveloped. In the sagittal plane, abnormal
conformation can best be described by the position of
the distal interphalangeal joint (DIP), either a flexural
 |
|
Fig. 2. Horse with one heel bulb displaced proximally (sheared
heel conformation). Note the contour of the pastern above the
displaced heel bulb. |
deformity or marked dorsiflexion (ie, extension)
of the joint. The shape or conformation of the hoof
in the sagittal plane will be dependent on the tension
in the deep digital flexor tendon, the integrity of
the laminar apparatus, and the digital cushion-all
of which determine the angle of the solar margin of
the distal phalanx. A flexural deformity will overload
the toe, whereas marked dorsiflexion of the DIP
joint will overload the palmar section of the foot.
4. Evaluation of the Hoof Capsule
A detailed morphological examination of the foot
should begin with observing the horse in motion,
both going away from and toward the examiner, on
a firm, flat surface to note the landing pattern.
The foot is then viewed from all sides while it is on
the ground. Finally, the ground surface is examined
with the foot off the ground. Additionally,
small changes in the shape of the hoof capsule (such
as the coronet and the digital cushion) may be better
appreciated by careful palpation of the foot than by
visual inspection.
 |
|
Fig. 3. Dorsal view: the hoof should be symmetrical. A line
drawn between any two comparable points on the coronary band
should be parallel to the ground. The hoof should be symmetrically
related to the distal limb such that a vertical line should
bisect the third metacarpal bone, the pastern, and the hoof (courtesy
of Dr Andy Parks). |
5. Dorsal Aspect
When the foot is viewed from the dorsal aspect, the
ideal hoof should be approximately symmetrical.
An imaginary line drawn between any two comparable
points on the coronary band should be parallel
to the ground. The medial wall should be the same
height as the lateral wall, but because it is often
slightly steeper, it may be slightly shorter. An
imaginary line that bisects the third metacarpal
should bisect a line drawn between any two comparable
points on the coronary band or the ground
surface of the hoof. Similarly, the hoof should be
symmetrically related to the distal limb such that an
imaginary line that bisects the third metacarpal
bone, bisects the pastern and the hoof, allowing for
the slight asymmetry caused by the different angles
of the medial and lateral wall (Fig. 3).1
When the
foot is viewed from the dorsal aspect, the shape of
the forefeet may be asymmetrical, with one hoof
being narrower than the other ("mis-matched feet").
Several abnormalities may be visible at the toe/
quarters such as flares or under-running of the wall.
The coronary band may be unevenly distributed,
most commonly by an uneven slope from one side of
the foot to the other. A distally directed arch in the
coronary band in the dorsal portion of the foot usually
indicates extensive remodeling of the distal phalanx
at the toe. Examination of the growth rings
below the coronet may show divergence of the rings
from one side to the other indicating uneven or excessive
load (Fig. 4). The angulation of the dorsal horn tubules toward the medial or lateral side of the
hoof capsule should be noted; normally they are
 |
|
Fig. 4. Note divulgence of growth rings below the coronet from
the lateral to medial side. |
parallel, so when they appear tilted medially or laterally,
it suggests that the whole hoof capsule may
be tilted in that direction (Fig. 5). The position of
where the pastern bisects the hoof capsule should be
noted, that is, is its entry on the midline or displaced
medially or laterally?
On palpation, the coronary band of a healthy hoof
should feel thick and spongy. There should be no
evidence of a "ledge" or "trough" behind the proximal
margin of the hoof capsule when palpated. A depression
in the coronary band indicates that the
distal phalanx has displaced within the hoof capsule,
a finding that can be present in sound horses.12
This palpable depression will generally be accompanied
by a thin, flat sole, narrow frog, and contracted
heels. The dorsal aspect of the coronary band
should also be palpated for effusion of the DIP joint.
This is often seen with horses that have a broken
back hoof-pastern axis.
 |
|
Fig. 5. Hoof with a separation in the dorsal hoof wall. Note the
angulation of the horn tubules toward the medial side of the
foot. Also note the focal "arch" in the coronet on the lateral side. |
6. Lateral Aspect
When viewed from the lateral aspect, the angle the
dorsal hoof wall forms with the ground is variable and typically related to the conformation of the digit.
The heel tubules of the hoof capsule should form an
angle with the weight bearing surface similar to the
angle of the horn tubules in the toe region. Tradition
has it that the angle of the wall at the heel
should match that of the dorsal hoof wall; however,
it is usually a few degrees less. As the foot accepts
weight, it expands and the ground surface at the
heels moves against the shoe, causing wear that
decreases the heel angle. The amount of wear is
dependent on the integrity of the structures in the
heel. The length of the dorsal hoof wall is similarly
variable but is determined by the amount of sole
depth present. There are two guidelines that relate
the proportion of the foot to the rest of the distal
limb.
 |
|
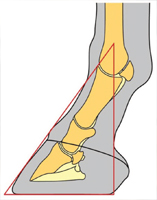
Fig. 6. Conformation of the foot as it relates to the digit can be
depicted with a triangle. A line drawn down the dorsal surface
of the pastern and hoof is the hoof-pastern axis. A vertical line
that bisects the third metacarpal bone should intersect the
ground at the palmar aspect of the heels of the hoof capsule.
Connect these two lines with the angle of the dorsal hoof
wall and the ground surface of the foot to form a triangle (courtesy
of Dr Andy Parks). |
First, the foot-pastern axis describes the relationship
between the angles made by the dorsal
hoof wall and the dorsal aspect of the pastern with
the ground. Ideally, the dorsal hoof wall and the
pastern form the same angle with the ground so that the angle between them is 180° and the axis is
considered straight. Second, an imaginary line
that bisects the third metacarpal should intersect
the ground at the most palmar aspect of the ground
surface of the hoof. These two guidelines used in
conjunction with the angle of the dorsal hoof wall
and the ground surface of the foot combine to form a
triangle of proportions that represents the relationship
between the hoof and the distal limb regardless
of the size of the horse (Fig. 6).1
Evaluation of the
hoof capsule from the side view should begin with
the coronet as this structure can provide very useful
information. The healthy coronary band should
have a gentle, even slope from the toe to the heels,
and the hair should lie flat against the hoof capsule;
hair projecting horizontally may indicate excessive
forces on the associated hoof wall.
13 The coronary
band is dynamic, and its shape can be affected by
chronic overloading.
14 A proximally directed diffuse
arch at the quarters or a focal directed arch
toward the heels is evidence of chronic overloading
of that section of the foot (Fig. 7). A coronary band
with an acute angle at the heels relative to the
ground that bends distally at the heel to form a
"knob" appearance is an indication that the foot has
poorly developed or under-run heels and the hoof
wall at the heels has migrated dorsally (Fig. 8).
 |
|
Fig. 7. A section of the coronet in the palmar section of the foot
has been displaced proximally (focal arch). Note the relationship
of the heel of the shoe and the origin of the defect, which
denotes excessive load. The foot on the right shows a change in
angulation of the horn tubules, curvature of the growth rings, and
a proximal displacement of the coronet (dorsal arch). |
 |
|
Fig. 8. Foot with under-run heels showing the "knob" appearance.
Note the curve in the growth rings as the heels migrate
dorsally. There will often be a depression ("thumbprint") showing
the extent the heels of the hoof capsule have migrated forward
(arrow). Palmar view shows the decrease in structural mass of
the digital cushion. |
 |
|
Fig. 9. Clubfoot. Note the coronary band has lost the slope and
is almost parallel with the ground. Also note the flare in the
dorsal hoof wall. |
A coronary band that is horizontal relative to the
ground and often accompanied by a flare in the
dorsal hoof wall would denote an upright or clubfoot
conformation (Fig. 9). Asymmetry of the height of the coronary band in the quarter/heel region on one
side occurs when the horse develops a "sheared
heel," a hoof capsule distortion resulting in proximal
displacement of one quarter/heel bulb relative to the
contralateral side of the foot.
15 The medial heel
bulb/quarter is more commonly displaced proximally,
as it is more common for the foot to be offset
laterally. The angle of the coronary band can be
used to estimate the position of the distal phalanx
within the hoof capsule. One study described the
angle of the coronary band of apparently normal
front feet to be 23.5° ± 3°.
16 If the angle of the
coronary band is >45°, the plane of the solar margin
of the distal phalanx will decrease. At the other
extreme, a coronary band parallel to the ground is
indicative of a high palmar angle, which is often
associated with a club foot or rotation of the distal
phalanx. The width of the growth rings below the
coronet should be equal from toe to heel. A disparity
in the width of the growth rings between the toe
and the heels is indicative of non-uniform circulation
of the coronary corium or excessive forces below
because wall growth is generally inversely related to
load. An example of this disparity would be chronic
laminitis typified by more horn growth at the heels than toe growth. However, regional irregularity in
spacing of growth rings is not uncommon; the most
frequently observed is a decrease in spacing at the
quarter associated with proximal displacement of
the coronary band as noted with sheared heels.10
The angulation of the horn tubules from dorsal to
palmar should be noted because horn tubules that
are parallel with the ground in the heel area are
associated with under-run heels. Flaring or concavity
of the dorsal hoof wall accompanied by underrunning
of the heels is readily appreciated from the
lateral side. The presence of hoof wall flares or
cracks are often caused by chronic, excessive overloading
of the hoof wall in the region in which these
defects are found.
10,11,14,17 Vertical cracks in the
quarter are more likely to occur with a sheared heel.
Horizontal cracks are usually the result of a disruption
of production of horn caused by coronary band
trauma or when a subsolar infection ruptures at the
coronary band.
7. Palmar Aspect
The heels are evaluated from the palmar aspect for
their overall width and height. The heels frequently
become narrowed when the foot itself is
narrow. Additionally, the central sulcus of the frog
may extend proximal to the hairline so that a cleft
becomes apparent in the skin of the pastern between
the heels. The overall height of the heels is readily
assessed from the lateral aspect, but viewing from
the palmar aspect is useful to compare the relative
heights of the two heels. For example, in the case
of the sheared heel, one heel is displaced proximally
in relation to the other. Another example is mismatched
feet in which there is a marked disparity in
heel height. The contour of the junction of the heel
bulbs with the skin can be evaluated relative to the
width of the hoof wall at the heels and the thickness
of the digital cushion (Fig. 10).
 |
|
Fig. 10. A, Illustration shows various contours of the junction of
the heel bulbs with the skin; B, wide heel; C, contracted heel with
a poor digital cushion. Note also the sheared heel on this foot. |
8. Distal or Solar Aspect
When viewed from the distal surface, the ground
surface of the foot should be approximately as wide
as it is long. The foot should be approximately symmetrical about the long axis of the frog; the
lateral side of the sole frequently has a slightly
greater surface area that corresponds with the difference
in wall angles at the quarters described in
the dorsal view. The width of the frog should be
approximately 60% to 70% of its length. The
ground surface of the heels should not project dorsal
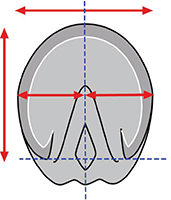
to the base of the frog. Imaginary lines drawn
across the most palmar weight-bearing surface of
the heels and across the heel bulbs at the coronary
band should be parallel and both lines should be
perpendicular to the axis of the frog (Fig. 11).
 |
|
Fig. 11. The ground surface of the foot should be approximately
as wide as it is long (red lines) and approximately symmetric
about the long axis of the frog (blue lines). The heels should not
project dorsal to the frog (courtesy of Dr Andy Parks). |
1
If a three-dimensional object such as the foot
changes in one plane, it will change in at least one
other plane. Therefore, examination of the ground
surface of the foot reveals much about the changes
in the wall of the hoof capsule. For example, if the
contour of the wall is displaced away or toward the
median plane in the dorsal two thirds of the foot,
this usually corresponds with a flare or under-running
of the wall, respectively. If only one heel buttress
is displaced dorsally in relation to the base of the frog, it usually corresponds with the proximal
displacement of that heel plus or minus the quarter
termed sheared heel.
The author begins the evaluation of the solar surface
of the hoof capsule by drawing a line across the
widest part of the foot. This line forms a consistent
landmark and is located just dorsal to the center of
rotation (of the distal interphalangeal joint). With
the use of this line as a starting point, there should
be approximate proportions from this line to the
perimeter of the toe and to the base of the frog (Fig.
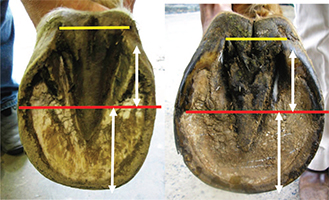
12).
 |
|
Fig. 12. Two examples of a line drawn across the middle or
widest part of the foot to determine proportionality (red line) by
use of the base of the frog (yellow line) and the perimeter of the
toe. White lines are the distance from the middle of the foot to
the end of the heel and to the toe, respectively. Note that both
heels have migrated dorsally and both frogs are receded below the
hoof wall. |
This creates a relative proportion from the
front of the foot to the palmar aspect that is related
to the alignment of the center of rotation in the
middle of the foot or, when shod, the middle of the
shoe. The normal solar surface of the foot may be
wider laterally than medially. The width of a
healthy frog should equal 60% to 70% of its length;
therefore, the width and length of the frog should be
critically evaluated using these guidelines.
1,8,18 The
untrimmed frog should be on the same plane with the
hoof wall at the heels; it should not be receded between
the hoof wall or protrude beyond the solar surface of
the hoof wall. In general, the frog is usually constant
in length, and its axis is almost always aligned with
the medial plane of the foot but its width is variable.
As the frog functions as an expansion joint, a decrease
in width is generally associated with contracture of
the hoof capsule at the heels. The frog of a healthy
hoof has sufficient depth at its dorsal aspect to reach
the bearing surface.
17 The relationship of the untrimmed
frog to the sole indicates the position of the
distal phalanx within the hoof capsule (ie, the angle of
the solar margin of the distal phalanx).
18 For instance,
if the apex of the frog is deeply recessed and the frog
appears to be angling toward the coronary band at the
toe, the distal phalanx is probably similarly positioned,
creating a negative palmar angle. The position of the heels of the hoof wall relative to the base of the
frog should be evaluated. Ideally, the most palmar
extent of the bearing surface of the heel tubules
would be at the base of the frog and very near a
vertical line drawn thru the middle of the third
metacarpal bone. When the ground surface of the
heels is dorsal to the base of the frog, the heels are
low, under-run and/or increased in length. The
structures of the heel (hoof wall, buttress, angle of
sole, bars) should be present and well-defined.
If the heels have migrated dorsally relative to the
frog and the structures are present, the heels are
considered low; if the structures of the heel are absent
or damaged, then the heels are considered under-
run. The bars of the heel should be straight as
curvature indicates contracted heels. The proportionality
of the foot dorsal to the widest part of the
foot should be evaluated. As the heels move forward,
 |
|
Fig. 13. A rasp is placed across the foot and a ruler is placed
within the collateral groove of the frog to measure the distance
between the deepest part of the groove and the plane of the solar
surface of the foot. This simple technique can be used to approximate
the sole depth (courtesy of Dr John Schumacher). |
there will generally be a substantial increase
in the proportion of the toe relative to the heels.
A long toe will also be accompanied by an increased
distance between the toe and the apex of the frog.
The sole-wall junction should be solid and compact.
Widening or fissures in the sole-wall junction and
hoof wall separations dorsal to the sole wall junction
occur with lengthening of the toe. The healthy sole
tends to be concave and callused adjacent to the sole
wall junction (white line). It should have a gradual
slope from the apex of the frog to the sole wall
junction and not a significant "trough." The sole
should be between 10 to 15 mm thick beneath the
margin of the distal phalanx and should not deform
when hoof testers are applied. A ruler calibrated in
millimeters can be placed within the collateral
groove of the frog to measure the distance between
the deepest part of the groove and the plane of the
solar surface of the foot. The consistent distance
(10 to 11 mm) between the distal phalanx and the
collateral groove depth at the apex of the frog allows
the clinician to predict sole depth. If one imagines
moving the ground plane proximally so that the
distance from the ground plane to the depth of the
collateral groove decreases, it becomes clear that
sole depth decreases as collateral groove depth decreases
13
(Fig. 13).
Horses with poor heel structure typically have a
poorly developed digital cushion and thin collateral
cartilages. These soft tissue structures determine
the overall conformation of the palmar portion of the
foot. Clinicians should gain an appreciation for
variation in the consistency and overall size of the
digital cushion and collateral cartilages. The digital
cushion can be palpated between a thumb placed
between collateral cartilages and the fingertips
placed on base of the frog. A sense of "normal" can
be acquired by palpating the digital cushions of
sound horses with "good feet" and comparing those
findings with those of horses with poorly conformed
feet. The depth of the combined tissues of normal
digital cushion and frog should be approximately 2
inches, but this can vary among different breeds.13 Horses with under-developed digital cushions typically
have low or under-run heels that lack stability
and can be easily distracted independently or they
may have contracted heels and narrow, non-weightbearing
frogs.19,20
9. Conclusions
The clinical examination of the equine foot has been
well-described and is generally performed in lameness
cases. Evaluation of the hoof capsule during
the lameness examination will provide additional
information as to the etiology and treatment of the
lameness but will also serve as a guideline to apply
therapeutic farriery and other preventive measures
to maintain a healthy hoof. The morphology of the
hoof capsule reveals deformation and changes in
growth that occurs after increased or reduced force.
The relationship between the limb and the foot indicate
conformations that predisposes the foot to
abnormal weight-bearing. Inversely, with the use
of abnormal distribution of forces and the subsequent
hoof capsule distortion as a template, appropriate
farriery or therapeutic farriery will form at
least part of the treatment plan. Here it is essential
to be familiar with the biomechanics of the foot
and how these forces can be altered to change the
distribution of forces or the focal stresses on a given
section of the foot.
References
- Parks AH. Form and function of the equine digit. Vet Clin N Am Equine 2003;19:285-307.
- Parks AH. Aspects of functional anatomy of the distal limb, in Proceedings. Am Assoc Equine Pract 2012;58:132-137.
- Johnston C, Back W. Hoof ground interaction: when biomechanical stimuli challenge the tissues of the distal limb. Equine Vet J 2006;38:634-641.
- Eliashar E. An evidence based assessment of the biomechanical effects of the common shoeing and farriery techniques. Vet Clin N Am Equine 2007;23:425-442.
- Parks AH. Therapeutic trimming and shoeing. In: Baxter GM, editor. Adams & Stashak's Lameness in Horses. 6th edition. West Sussex: Wiley-Blackwell; 2011:986-992.
- Turner TA. The use of hoof measurements for the objective assessment of hoof balance, in Proceedings. Am Assoc Equine Pract 1992;38:389-395.
- Redden RF. Hoof capsule distortion: understanding the mechanisms as a basis for rational management. Vet Clin N Am Equine 2003;19:443-462.
- O'Grady SE, Poupard DA. Physiologic horseshoeing: an overview. Equine Vet Edu 2001;13:330-334.
- Castelijns HH. The basics of farriery as a prelude to therapeutic farriery. Vet Clin N Am Equine 2012;28:316-320.
- O'Grady SE, Castelijns, HH. Sheared heels and the correlation to spontaneous quarter cracks. Equine Vet Edu 2011; 23:262-269.
- O'Grady SE. How to manage sheared heels, in Proceedings. Am Assoc Equine Pract 2005;51:451-456.
- Turner TA. Examination of the equine foot. Vet Clin N Am Equine 2003;19:309-332.
- Schumacher J, Taylor D, Schramme MC, et al. Localization of pain in the equine foot emphasizing the physical examination and analgesic techniques, in Proceedings. Am Assoc Equine Pract 2012;58:138-155.
- Turner TA. Predictive value of diagnostic tests for navicular pain, in Proceedings. Am Assoc Equine Pract 1996;42:201-204.
- Dabareiner RM, Moyer WA, Carter GK. Trauma to the sole and wall In: Ross MW, editor. Diagnosis and Management of Lameness in the Horse. 2nd edition. St Louis: Elsevier Saunders; 2011:309-319.
- Eliashar E, McGuigan MP, Wilson AM. Relationship of foot conformation and force applied to the navicular bone of sound horses at the trot. Equine Vet J 2004;36:431-435.
- Booth L, White D. Pathological conditions of the external hoof capsule In: Floyd AE, Mansmann RA, editors. Equine Podiatry. St Louis: Saunders Elsevier; 2007:224-252.
- Dabareiner RM, Carter GK. Diagnosis, treatment and farriery for horses with chronic heel pain. Vet Clin N Am Equine 2003;19:417-441.
- Bowker RM. The concept of the good foot: its evolution and significance in a clinical setting. In: Ramey P, editor. Care and Rehabilitation of the Equine Foot. Lakemont, Georgia: Hoof Rehabilitation Publishing LLC; 2011:2-34.
- Moyer WA, Carter GK. Examination of the equine foot. In: Floyd AE, Mansmann RA, editors. Equine Podiatry. St Louis: Elsevier Saunders; 2007:112-127.