How to Construct and Apply the Wooden Shoe for Treating Three Manifestations of Chronic Laminitis
Reprinted with permission from the American Association of Equine Practitioners.
Originally printed in the 2007 AAEP Convention proceedings
Stephen E. O'Grady, BVSc, MRCVS; Micheal L. Steward, DVM; and Andrew H. Parks, VetMB, MRCVS, Diplomate ACVS
Authors' addresses: Northern Virginia Equine, PO Box 746, Marshall, Virginia 20116 (O'Grady);
Shawnee Animal Hospital, 1509 North Kickapoo Street, Shawnee, Oklahoma 74804 (Steward); and
Department of Large Animal Medicine, College of Veterinary Medicine, University of Georgia,
Athens, GA 30602 (Parks); e-mail: sogrady@look.net. © 2007 AAEP.
1. Introduction
The treatment of chronic laminitis presents a challenge
to veterinarians, farriers, and horse owners.
Our ability to rehabilitate horses with laminitis,
regardless of the method of treatment, is related to
the severity of damage to the lamellae. Chronic
laminitis is defined by the presence of mechanical
collapse of the lamellae and displacement of the
distal phalanx within the hoof capsule.1 Two forms
of displacement of the distal phalanx are widely
recognized: dorsal capsular rotation (the most
common form of displacement) and distal displacement.
Recently, two of the authors (AHP and SEO)
have become more aware of the rotation that occurs
in a medial or lateral direction where the distal
phalanx displaces distally on one side. If dorsal
capsular rotation is severe, the instability of the
distal phalanx combined with the weight of the
horse often leads to prolapse of the sole or prolapse
of the distal phalanx through the sole. Recently,
the wooden shoe has emerged as the most consistently
successful method to address these three entities
of chronic laminitis and are used extensively
by two of the authors (SEO and MLS).2 The
wooden shoe allows the distal phalanx to be realigned.
It has all the mechanical advantages of
the other shoes previously advocated for the treatment
of laminitis, because it addresses the forces
exerted on the compromised lamellae. Additionally,
it is able to concentrate weight bearing evenly
over a specified section of the foot because of its flat,
solid construction. The major advantages of the
wooden shoe are that it is easy to construct, it is
applied in a non-traumatic manner, and it can easily
be altered according to the radiographic appearance
and structural requirements of each individual
foot/horse.
2. Radiology
The lateral radiograph has always been considered
the "gold" standard for evaluating chronic laminitis,
but it does not allow for identification of asymmetrical
medial or lateral distal displacement. Therefore,
the authors consider it crucial that a
dorsopalmar (dorso 0° palmar) radiographic projection is included as part of the radiographic study for
either acute or chronic laminitis. High-quality radiographs
are required to visualize the osseous
structures within the hoof capsule as well as the
hoof capsule itself. Radio-opaque markers can be
used to determine the position of the distal phalanx
in relation to surface landmarks.
The radiographic features of chronic laminitis are
well documented.3 The following observations
from the lateral radiograph are important in determining
the prognosis and guiding treatment: the
thickness of the dorsal hoof wall, the degree of dorsal
capsular rotation, the angle of the solar surface of
the distal phalanx relative to the ground, the distance
between the dorsal margin of the distal phalanx
and the ground, and the thickness of the sole.
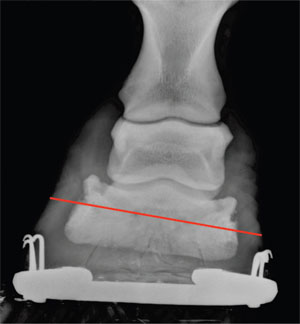 |
| Fig. 1. Radiograph of asymmetrical downward displacement of the distal phalanx on the medial side. Note that the line drawn through the solar foramens is not parallel with the ground. Also note the disparity in the joint space from the lateral to the medial side. |
 |
| Fig. 2. The basic wooden shoe where the proximal piece is cut vertical, and the thicker piece is cut on a 45° angle. Note the wedge pad attached to the wooden shoe for heel elevation, if necessary. |
The dorsopalmar radiograph is examined to determine
the position of the distal phalanx in the frontal
plane. Asymmetrical distal displacement of the
distal phalanx on either the lateral or medial side is
present if an imaginary line drawn across the articular
surface of the distal interphalangeal joint or
between the solar foramens of the distal phalanx is
not parallel to the ground, if the joint space is widened
on the affected side and narrowed on the opposite
side, or if the width of the hoof wall appears
thicker than normal on the affected side. If the
position of the coronary band is visible on the radiograph,
then the distance between the coronary band
and the palmar processes of the distal phalanx will
be greater on the affected than the unaffected side
(Fig. 1).
3. Materials and Methods
Construction of the Shoe
The authors chose wood because its light weight, the
ease with which it can be shaped (both before and
after application), and its ability to dissipate energy
at impact while remaining rigid.4 The basic shoe is
made from two pieces of plywood. An aluminum
shoe with a broad toe that is available in sizes 00-5
is used as a template.a One piece of plywood is
0.250-0.375 in thick, and the second piece is 0.75 in
thick. Using the aluminum shoe as a template, the
thinner piece of plywood is cut out with a vertical
border, and the thicker piece is cut out with a border
beveled at a 45° angle using an angle saw.b As a
modification to the basic pattern, the palmar or heel
section of the wooden shoe can be cut at a 15°, 30°, or
45° angle or left straight, if desired. The pieces of
plywood are glued together; the thinner portion is
proximal, and two 1-in drywall screws are used to
secure the two pieces together. A wood rasp is used
to blend the cut angles into a uniform slope (Fig. 2).
 |
Fig. 3. Wooden shoe fabricated from a single piece of plywood.
Note the recess in the foot surface of the shoe created with a router. |
 |
| Fig. 4. Proximal section of plywood cut in the shape of a "W." Note the 3° wedge to elevate the heels. |
The shoe can also be fabricated from a single piece
of 1.125-in plywood (purchased as subflooring plywood).
If the sole or distal phalanx is prolapsed, a
recess can be created in the proximal surface of the
shoe by cutting a half-moon shape dorsal to a line
that is one-third the length of the shoe in the thinner
piece of plywood with a router. A hand grinder can
be also used to create a trough in the shoe below the
area of the sole or bone that has prolapsed (Fig. 3).
The same end can be achieved by cutting the thinner
piece in the shape of a "W" and then attaching it
to the thicker section of plywood as described above
(Fig. 4).
Goals of Treatment for Chronic Laminitis
Trimming and shoeing has always been the "mainstay"
of treating chronic laminitis, and it is directed
at reducing/removing the adverse forces on the compromised
lamellae. In considering hoof care in
horses with chronic laminitis, there are three goals
for therapy: to stabilize the distal phalanx within
the hoof capsule, to control pain, and to encourage
new hoof growth to assume the most normal relationship
to the distal phalanx possible. Realignment
of the third phalanx to create a better
relationship of the solar surface of the distal phalanx
with the ground is used as the basis for treating
chronic laminitis.5-7 Applying the wooden shoe after
this procedure compliments the realignment of
the distal phalanx and further decreases the forces
on the lamellae. The same shoeing principles for
other methods are applied to the wooden shoes that
are used to treat chronic laminitis. They are to
recruit ground surface, to reposition the breakover
palmarly, and to provide heel elevation as needed.5
 |
Fig. 5. Lateral radiograph showing dorsal capsular rotation.
Note the lack of hoof-wall growth at the coronet at the toe. The red arrow denotes the center of articulation. The black line shows the amount of heel to be removed. |
Dorsal Capsular Rotation
Dorsal capsular rotation describes the divergence of
the dorsal hoof wall from the dorsal parietal surface
of the distal phalanx independent of the relationship
of the distal phalanx with the phalangeal axis.8
A generalized outline will be used to describe the
preparation of the foot and application of the wooden
shoe for this type of displacement; it must be noted
that each case of chronic laminitis must be treated
on an individual basis. The foot must be trimmed,
and the shoe must be sized and positioned in relation
to the underlying distal phalanx, regardless of
the conformation of the hoof. Therefore, measurements
must be made from radiographs taken before
shoeing. Using the radiograph for guidance, a vertical
line is drawn from the center of the distal end
of the second phalanx to the ground. This line
should correspond to the widest part of the foot.
A line is then drawn parallel to the solar border of
the distal phalanx starting 15 mm below the palmar
process of the distal phalanx and continuing dorsally.
The hoof wall to be removed in the heel area
can be determined from the mass below this line
(Fig. 5).5-7
A line is drawn across the widest part of the foot
and the hoof wall; the area palmar to this line is
trimmed according to the lines drawn on the radiograph.
If, as is frequently the case, the wall and
sole dorsal to the line drawn across the sole is <15mm, trimming in this manner will create two different
planes on the ground surface of the foot. A line
is also drawn across the center of the wooden shoe
(Fig. 6).
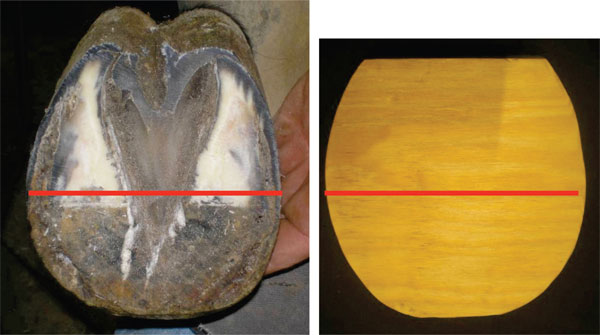 |
| Fig. 6. Using the widest part of the foot as a guideline (red line), the heels are trimmed in a palmar direction. The red line drawn in the middle of the wooden shoe is used to determine the proper size wooden shoe to use. |
The correct size of the shoe is determined by placing
the lines on the foot and the shoe on top of each
other; the appropriate size shoe will extend from the
line drawn across the foot to the end of the heel or 6-8
mm palmar to the heel. To compensate for the
increase in tension in the deep digital flexor tendon
that is caused by lowering the heels of the hoof
capsule, the heels can be raised by applying a wedge pad to the hoof surface of the wooden shoe. The
angle of the wedge is usually 2-4°, depending on the
amount of heel horn removed. The wedge pad is
attached to the shoe with 1-in drywall screws.
Using a 0.078-in drill, a guide hole is drilled through
the lateral and medial side of the hoof wall at the
widest part of the foot, and a 1.5-in drywall screw is
placed in each hole and screwed in until just visible
on the ground surface of the foot. To better increase
weight bearing by the sole, bars, frog, and
sulci, a deformable impression materialc is applied
to the solar surface of the foot. The shoe is now
placed on the ground surface of the foot and attached
using 2-in drywall screws. The foot is placed on the
ground and allowed to bear weight; this allows the
impression material to set between the foot and the
shoe in the optimal form. Two to three more holes are drilled through both sides of the hoof wall, and
the shoe is secured in place using additional screws.
If the mass of the hoof wall is insufficient or if the
quality of the hoof wall is insufficient to hold the
screws, screws can be placed in the wooden shoe
against the available hoof wall to act as struts, and
an acrylic composited is used to form a bond between
the hoof wall, screws, and wooden shoe. With the
foot on the ground, a vertical line is drawn from the
dorsal coronet to the ground. The point where the
line meets the ground is where the breakover point
of the shoe should be positioned (Fig. 7).
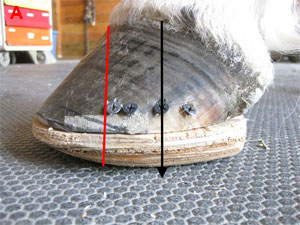 |
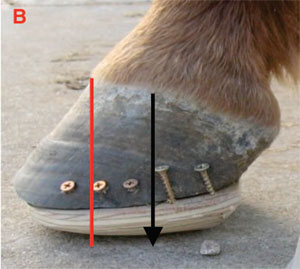 |
| Fig. 7. (A) A wooden shoe with impression material and a wedge pad to provide heel elevation. The black arrow is the widest part of the foot. The red line denotes the point of breakover on the ground surface of the shoe. (B) A wooden shoe fabricated from a single piece of plywood with the same guidelines as A. |
This point will usually be just dorsal to the margin
of the distal phalanx. Setting the breakover to this
point in the shoe is easily accomplished using a hoof
rasp with the foot being held in the farrier position.
Deep digital tenotomy has been the recommended treatment when prolapse of the distal phalanx has
occurred secondary to dorsal capsular rotation.
One author (SEO) has observed that the wooden
shoe has provided an alternative and often better
means to treat this condition without surgery.
 |
| Fig. 8. Left forelimb with distal phalanx offset toward the medial side. |
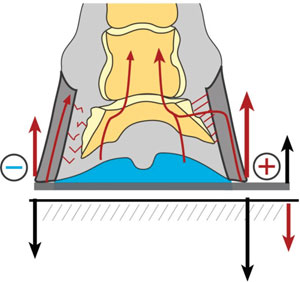 |
| Fig. 9. Diagrammatic illustration of the method used to move the forces toward the unaffected side. |
Medial or Lateral Asymmetrical Displacement of the Distal Phalanx
In displacing asymmetrically, the distal phalanx rotates
in the frontal plane within the hoof capsule
and moves away from the hoof wall on the affected
side. The reason that some horses displace asymmetrically
is not completely understood. Clinical
observations by two of the authors (SEO and AHP)
suggest that asymmetrical displacement is usually
toward the medial side, and the distal phalanx
within the hoof capsule is usually offset toward the
affected side (Fig. 8).
Occasionally, these two authors have observed
distal displacement laterally in instances where the
horse developed laminitis in one foot after prolonged
weight bearing subsequent to severe lameness in the
contralateral limb. Aside from general trimming of
the foot, removal of hoof wall at the heels may not be
necessary. The sizing of the shoe and the application
of impression material will be the same as described
for dorsal capsular rotation. The crucial
difference between treating medial or lateral asymmetrical displacement compared with dorsal capsular
displacement is the mediolateral positioning of
the shoe. Based on the apparent asymmetry of the
distal phalanx within the hoof capsule visible on
radiographs, a clinician's first response might intuitively
be to try and restore the asymmetry of the
distal interphalangeal joint and the position of the
distal phalanx in relation to the ground. This
would most readily be accomplished by raising the
side of the hoof on which the distal phalanx is displaced.
However, this will increase the weight
bearing on the affected side and cause the distal
phalanx to displace further in relation to the hoof
capsule, which will increase the pain. Therefore,
the appropriate technique is to decrease weight
bearing by the affected wall, which is accomplished
by sharing weight bearing with the sole and frog and
increasing weight bearing with the unaffected wall.
This can be achieved by placing an extension on the
unaffected side (Fig. 9).
Because of its flat solid surface, the wooden shoe
combined with impression material seems to load
those structures away from the affected side. The
width of the hoof wall on the affected side is reduced
using a rasp on the outer surface. The wooden shoe
is then fitted so that the edge of the shoe is even with
or just under the hoof wall on the affected side, and
the shoe forms an extension of ~0.25-in beyond the
hoof wall on the unaffected side (Fig. 10).
If insufficient hoof wall is present on the affected
side to accommodate screws, screws can be placed
into the wooden shoe on an angle so that they lie
against the hoof wall. They should be bonded with
an acrylic composite.
 |
| Fig. 10. (A) Wooden shoe fitted with an extension on the lateral side. Note the screws that are inserted as struts to attach the shoe to the hoof wall with acrylic. (B) Wooden shoe with extension being attached to foot with screws. |
Prolapse of the Sole or Distal Phalanx
For prolapse of the distal phalanx, the foot is
trimmed to establish realignment, and heel elevation
is applied to the shoe to decrease the forces on
the deep digital flexor tendon. Before applying the
shoe, the wooden shoe is placed against the ground
surface of the foot and pressed against the exposed
corium of the distal phalanx. The moisture of the
tissue or a suitable dye applied to the corium will
create an impression on the foot surface of the
wooden shoe. A router can be used to cut out the
impression, or a trough can be created with a
grinder. The shoe is now applied, making sure that
the impression material is concentrated palmar to
the apex of the frog. The affected area can be
packed with an appropriate antiseptic from the front
of the shoe.
4. Results
Success of any given treatment for chronic laminitis
is hard to evaluate because of the individual diversity
between each case. In reviewing the records on
horses with the three types of displacement described
in this paper, the authors established basic
guidelines to evaluate the response after application
of the wooden shoe. All evaluations were for a period
of 8 wk post-application of the wooden shoe.
All three types of displacement were evaluated for a
decrease in the level of pain. To better evaluate the
wooden shoe for dorsal capsular rotation, the authors
chose cases that had been treated previously
with other methods of farriery with minimal response.
Increased hoof-wall growth at the coronet
at the toe and an increase in sole depth were used on
horses where the wooden shoe was applied for dorsal
capsular rotation. Increased hoof-wall growth at
the coronet on the affected side of the foot was used
for horses with unilateral displacement. Finally,
cornification of the exposed corium of the distal phalanx
as well as hoof-wall growth was used on those
cases where the distal phalanx had penetrated
through the sole.
| Table 1. |
| Type of Displacement |
Number of Cases |
Favorable Response |
% |
| Dorsal capsular rotation |
21 |
17 |
81 |
| Asymmetrical displacement |
11 |
8 |
65 |
| Penetration of distal phalanx through the sole |
9 |
7 |
77 |
There were 21 cases of dorsal capsular rotation,
and 17 (81%) had a favorable response to wooden
shoes. There were 11 cases of asymmetrical displacement,
and 8 (65%) had a favorable response to
wooden shoes. There were 9 cases of penetration
of distal phalanx through the sole, and 7 (77%) had
a favorable response to wooden shoes.
5. Discussion
The wooden shoe provides another very consistent
farriery option when treating a horse with chronic
laminitis. Removing the stresses on the lamellae
has always been difficult when using traditional
shoes to treat chronic laminitis. Traditional shoes
are placed under the hoof wall, which concentrates
the load on the compromised lamellae. The plane
of the wooden shoe combined with the impression
material allows the foot to become load sharing,
because the load is shared by the hoof wall and the
soft-tissue structures of the foot. Furthermore, cutting
the perimeter of the wooden shoe at a 45° angle
around the circumference of the foot is thought to
decrease the torque on the lamellae.6 Creating a
recess in the shoe under the distal phalanx in the toe
area relieves the load on the bone, and then, the
weight-bearing function is concentrated in the palmar
section of the shoe. When displacement of the
distal phalanx within the hoof capsule is severe, the
wooden shoe can be used as a transient treatment to
build sufficient hoof mass for the application of a
more conventional shoe.
References and Footnotes
- Hood DM. The mechanisms and consequences of structural failure of the foot. In: Hood DW, ed. The veterinary clinics of North America, vol. 15:2. Philadelphia: W.B. Saunders Co., 1999;437-461.
- Steward ML. How to construct and apply atraumatic therapeutic shoes to treat acute or chronic laminitis in the horse, in Proceedings. 49th Annual American Association of Equine Practitioners Convention 2003;337-346.
- Redden RF. Clinical and radiographic examination of the equine foot, in Proceedings. 49th Annual American Association of Equine Practitioners Convention 2003;174-185.
- Reid SR. Impact energy absorbing mechanisms in crushing and indentation of wood, in Proceedings. IUTAM Symp On Imact Dynamics 1994.
- O'Grady SE. Realignment of P3—the basis for treating chronic laminitis. Equine Vet Edu 2006;8:272-276.
- Parks AH. Chronic laminitis. In: Robinson NE, ed. Current therapy in equine medicine, vol. 5. St. Louis: W.B. Saunders Co., 2003;520-528.
- Parks AH, O'Grady SE. Chronic laminitis: current treatment strategies.In: O'Grady SE, ed. The veterinary clinics of North America, vol. 19:2. Philadelphia: W.B. Saunders Co., 2003;393-416.
- O'Grady SE, Parks AH, Redden RF, et al. Glossary of podiatry terms. Equine Vet Edu 2007;(in press).
- Natural Balance Shoe, EDSS, Penrose, CO 81240.
- Craftsman Angle Saw, Sears, Roebuck and Co., Hoffman Estates, IL 60179.
- Equilox Pink Impression Material, Equilox International, Pine Island, MN 55963.
- Equilox Adhesive System, Equilox International, Pine Island, MN 55963.
|