| Thirty years of laminitis research – what have I learned? Professor Christopher Pollitt Emeritus Professor of Equine Medicine Australian Equine Laminitis Research Unit School of Veterinary Science The University of Queensland Australia Reprinted with permission from the Equi-Meeting Maréchalerie. Original printed in the 2019 meeting proceedings, Haras National du Pin, France Introduction. In 1996 I published a paper entitled “Basement membrane pathology: a feature of acute equine laminitis”.1 This focussed attention on the lamellar dermal/epidermal junction and proposed for the first time that laminitis was characterised by disintegration of the lamellar interface. Other authors have cited the paper 178 times. This description of pathological anatomy required a thorough understanding of normal anatomy and consequently, studies of equine foot anatomy and pathology continued in tandem ever since. The lamellar interface is a key part of the suspensory apparatus of the distal phalanx or SADP and exploring it in detail enhanced my understanding of the laminitis process. Pathological disintegration of the SADP is the hallmark event of all laminitis pathology. Without the distal phalanx (DP) properly attached to the inside of the hoof, the weight of the horse and the forces of locomotion drive the bone down into the hoof capsule causing it to sink – sometimes slightly (with mild clinical signs) sometimes grossly (with severe clinical signs). The orientation of the SADP suggests that sinking of the DP, to a lesser or greater degree, must always occur at the onset of laminitis. During locomotion the hoof capsule is levered away (dorsally) from the distal phalanx resulting in ’capsular’ rotation. With DP dislocation important arteries and veins are sheared and crushed and the dermis of the coronet and sole is damaged. There is unrelenting pain in the feet and a characteristic lameness. 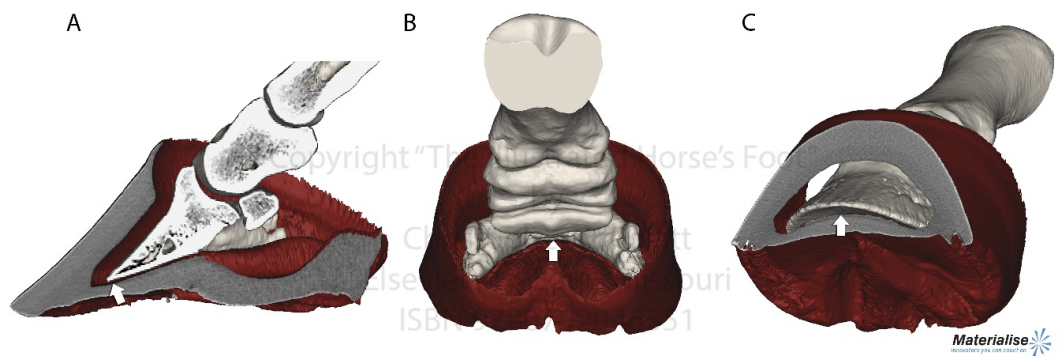 Fig. 1. 3D model of the front foot from a colitis affected mare with severe, rapid onset laminitis. Apart from the abnormal distance between them the anatomical relationship between the dorsal distal phalanx (DP) and the hoof capsule is near normal. There is no obvious rotation of either the dorsal hoof or DP. However, the DP margin is in abnormal close contact with the sole. The arrows, in A, B and C, show the absence of the ‘space’, 2 in life the dermis, normally between the distal phalanx and the horny sole. The DP distal margin, in contact with the sole, crushes the solear dermis causing severe pain. With each step the horse attempts, hoof ‘breakover’ levers the bone down on to the contused dermis. Hence the laminitis gait; shuffling, with the feet kept forward to avoid the posterior, breakover phase of the stride. Copyright ‘The Illustrated Horse’s Foot’ by Christopher C. Pollitt. Elsevier. St Louis. ISBN: 9780702046551. SADP disintegration begins surprisingly early in the developmental phase of laminitis. We have investigated the timeline of the basement membrane zone (BMZ) degradation sequence using serial biopsies. The molecular conformation of the lamellar basement membrane is altered 12 hours after dosing with oligofructose and a major constituent of the basement membrane, collagen IV, begins to disappear.2 Previously, damage to the lamellar basement membrane was attributed to MMP release and activation and I promoted this concept for many years. 3 However, I have had to change my mind. New evidence places MMP activation many hours later than other molecular events4 and MMP activation is no longer considered a primary trigger for laminitis. Indeed, our recent study blocking MMP activity, as laminitis developed, with potent MMP inhibitors, infused directly into lamellar tissue fluid made no difference to the outcome; laminitis pathology developed unabated in both treated and control (untreated) horses. MMP activation appears to be a downstream event, a response to injury not the cause of it. Our 1998 research suggesting that dilation of the foot vasculature was associated with laminitis development was ignored for many years.5 Long held dogma to the contrary is overturned by our recent studies. Perturbations in lamellar blood flow (ischaemia) play no role in the development of sepsis or hyperinsulinemia (HI) related laminitis (supporting limb laminitis is a different matter). Using microdialysis probes inserted directly into the lamellar milieu our recent studies show increased lamellar perfusion (hyperaemia) during the development phase. 6 Thus there is no rationale for the use of vasodilator drug therapy during the development phase of laminitis. Changes in the lamellar epidermal basal cell (LEBC), observed in lamellar tissues from experimental and clinical cases of laminitis, suggest that the LEBC is the primary target of SADP disintegration. The LEBC, robust and trouble-free in the healthy horse, may be the weak link in the hierarchy of tissues constituting the SADP, an intact “chain” counteracting substantial physical forces that will fail should one “link” give way. LEBC pathology. The first way that LEBC impairment can lead to DP descent is for LEBCs to dis-attach from their underlying basement membrane. This well documented mechanism 1,2,7,8 is clearly seen in experimental models (e.g. alimentary carbohydrate overload) and in clinical cases of sepsis-related laminitis (Fig 2). 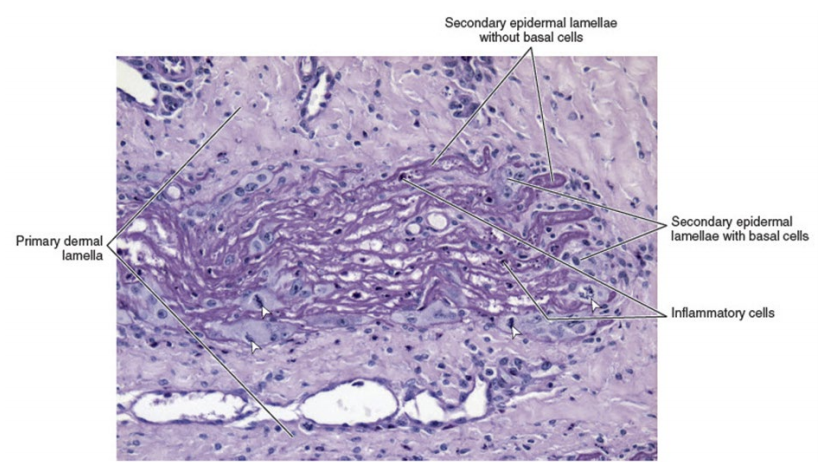 Fig 2. Photomicrograph of the axial tip of a midwall lamella from a colitis-affected mare with severe, rapid onset laminitis (Fig 1). The lamellar basement membrane is coloured magenta by periodic acid Schiff staining. Most of the secondary epidermal lamellae have lost their detached basal and parabasal cell populations, leaving only the empty basement membrane embedded in the dermis. However, a few basal cells survived and the numerous mitotic figures (arrowheads) among their nuclei suggest epidermal proliferation is underway. Many inflammatory cells have infiltrated the damaged lamellae. (Stain = periodic acid Schiff. Bar = 150 μm). Copyright ‘The Illustrated Horse’s Foot’ by Christopher C. Pollitt. Elsevier. St Louis. ISBN: 9780702046551. The second way that LEBC impairment can lead to DP descent is a more recent finding from hyperinsulinemia (HI) laminitis. LEBCs and secondary epidermal lamellae appear to weaken and stretch. 9-12This leads to SEL thinning and lengthening (Fig 3) without wholesale dis-attachment from the BM but with the same net result – the DP pathologically descends towards the solar dermis. 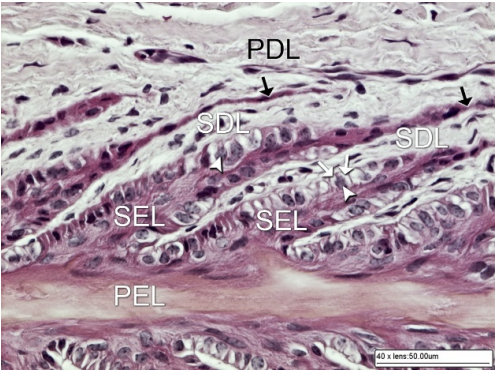 Fig 3. Histopathology of laminitis induced by 48 h hyperinsulaemia in an adult Standardbred (transverse section). The areas of clear cytoplasm (white arrows) beside the nucleus (arrowheads) bordering the lateral walls of most of lamellar epidermal basal cells suggest collapse of the actin cytoskeleton. However, the keratin intermediate filament cytoskeleton, an eosinophilic band between the nucleus and the basal plasma membrane, is still intact suggesting that hemidesmosomes in some cells have survived. As a result of cytoskeleton and attachment plaque degradation the tips of many secondary epidermal lamellae (SELs) are extremely attenuated and stretched into fine threads (black arrows). Stain = haematoxylin and eosin. Bar = 50 µm. Copyright Pollitt, C. C. 4 (2017). Dysregulation of the lamellar basal epithelial cell in laminitis: role of the cytoskeleton and cell junctions. Equine Laminitis. J. Belknap and R. Geor. Iowa, USA, John Wiley and Sons: 167-175. The initial loss of cell/cell and cell/basement membrane attachments untethers the cytoskeleton and destabilizes the LBEC nucleus causing it to change its shape and position. More profound loss of cell/cell and cell/basement membrane attachments likely further destabilises the SADP’s ability to counteract the strain of the horse’s body weight and allows the DP to descend into the hoof capsule. Changes in SEL dimensions are common to both sepsis and HI related forms of laminitis; SELs became longer and narrower. 10-12 HI-induced laminitis in ponies resulted in a doubling of SEL length in some lamellar regions. SEL narrowing and stretching occur as early as 6 h post experimental HI and 12 h post carbohydrate overload. Dysregulation of the LBEC cytoskeleton and its associated cell adhesion complexes including cytolink protein depletion, attachment plaque degradation and cytoskeletal collapse likely explain this sudden LBEC stretching and SEL lengthening. Significant decreases in cytolink protein and gene expression and associated LBEC cytoskeletal disorganisation have recently been reported in both HI- and CHO-induced laminitis.13,14 The LBEC is profoundly changed as laminitis-related pathology casts its shadow over the lamellar interface. Experimental models of equine laminitis and studies in other species have confirmed that aberrant cell signalling results in cell junction disassembly, loss of cell– cell and cell-matrix contacts and disruption in overall cell integrity. Ultimately, all this is due to disorganization of the physical inner framework of the cell, the cytoskeleton. Since the LBEC, the cornerstone of the suspensory apparatus of the distal phalanx, is constantly loaded, it is now understandable why LBEC dysregulation leads to downwards dislocation of the distal phalanx and its attendant signs of clinical laminitis. Two seemingly disparate causes of laminitis (sepsis and hyperinsuliaemia) not only show some of the same histologic changes (e.g. stretching of the secondary epidermal lamellae), but also growth factor signalling associated with disruption of cell adhesion properties in other species. The attack by laminitis on the LBEC that leads to loss of the protein components of the SEL cell adhesion complexes resembles changes occurring in skin cancer development. Anticancer drugs, currently in development, may be effective in preserving LEBC cell adhesion complexes and in turn SELs and the integrity of the SADP. 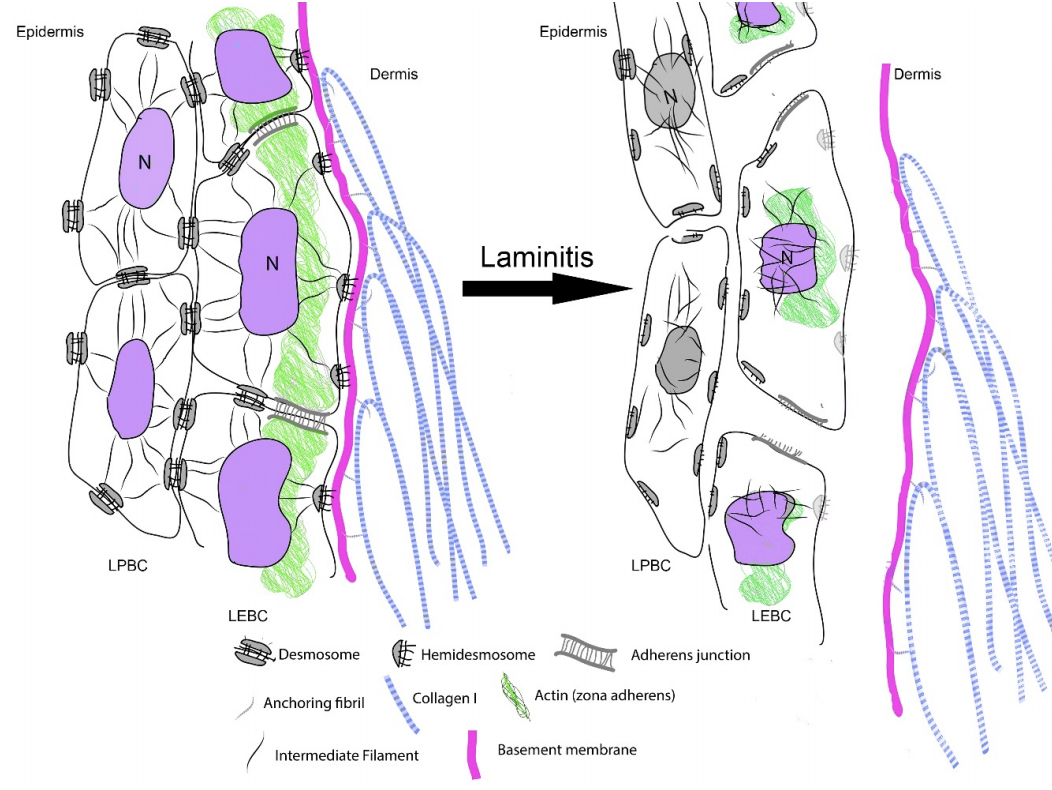 Fig 7. Schematic diagram of the cytoskeleton and major cell junctions of lamellar epidermal basal cells (LEBC). Hemidesmosomes attach LEBCs to the basement membrane via anchoring filaments. Desmosomes and adherens junctions connect adjacent cells via transmembrane cadherins. Keratin intermediate filaments span the cytoplasm linking the nucleus to hemidesmosomes and desmosomes. Actin links to adherens junctions via βcatenin and forms the zona adherens, a broad belt of interconnected, contractile actin filaments that encircles the lateral walls of each LEBC. On the dermal side of the basement membrane, bundles of collagen I connect to the basement membrane via hook-like anchoring fibrils (collagen VII). With the aberrant cell signalling of laminitis, hemidesmosomes no longer attach LEBCs to the basement membrane; cleaved anchoring filaments release the basement membrane and mechanical loading draws it downwards and away. Desmosomes and adherens junctions no longer connect adjacent cells as transmembrane cadherins have been lysed. Keratin intermediate filaments are free in the cytoplasm as links to hemidesmosomes and desmosomes via the cytolinkers plectin and desmoplasia have been degraded. Down regulation of β-catenin disintegrates the link between actin and the adherens junctions causing the zona adherens to disintegrate. Without functional cell junctions and with weakened attachment to the basement membrane LEBCs stretch and separate from each other and the basement membrane LPBC = lamellar parabasal cell. N = nucleus. Acute to chronic laminitis The disintegration of the SADP is initially invisible to the naked eye. With the passage of time however hoof changes occur as internal pathology alters growth patterns 6 and distorts hoof shape (Fig 8). If lameness persists and worsens there is likely on-going displacement of the distal phalanx relative to the hoof capsule and lysis of its cortex.  Fig 8. Pony with hyperinsulinemia laminitis of 10 weeks duration. The deep groove (arrowheads) in the dorsal hoof wall developed shortly after laminitis onset. The normally parallel hoof growth rings converge dorsally. Compared with the quarters and heels, hoof growth in the dorsal half of the hoof appears retarded. However, the dorsal hoof wall is in fact kinked and deformed and producing normal amounts of tubular horn out of sight. Copyright ‘The Illustrated Horse’s Foot’ by Christopher C. Pollitt. Elsevier. St Louis. ISBN: 9780702046551. Ultimately it is the strength of the SADP that determines prognosis. Many horses relapse after the initial laminitis episode despite early signs of improvement. We studied laminitis affected tissue, 7 days after the initiating episode, to assess the healing response to the disease. 15 Surprisingly, 7 days after laminitis, the destructive processes that caused lamellar basement membrane (BM) dysadhesion and lysis, basal cell dislocation and lamellar attenuation had abated. All epidermal compartments had normal appearing BMs and the majority of lamellar epidermal basal cells (LEBCs) were of normal shape and orientation. However lamellar anatomy was in disarray. The rows of organised, symmetrical hoof wall lamellae that characterize normal lamellae had been replaced with epidermal strands and islands, many no longer connected to their respective primary hoof wall lamellae. Laminitis, observed 7 days after induction, had reduced the surface area of the lamellar attachment apparatus and weakened it. Premature resumption of athletic exercise and thus greater foot break-over strain, particularly in the fore feet, could rupture surviving lamellar attachments. This is the likely mechanism behind recrudescent laminitis in apparently recovered horses. The disconnect between epidermal strands and islands (that 7 used to be functional SELs), and the keratinised axis of the PEL is semi-permanent and is found in sections of chronic laminitis weeks and months after the initial incident (Fig 9). 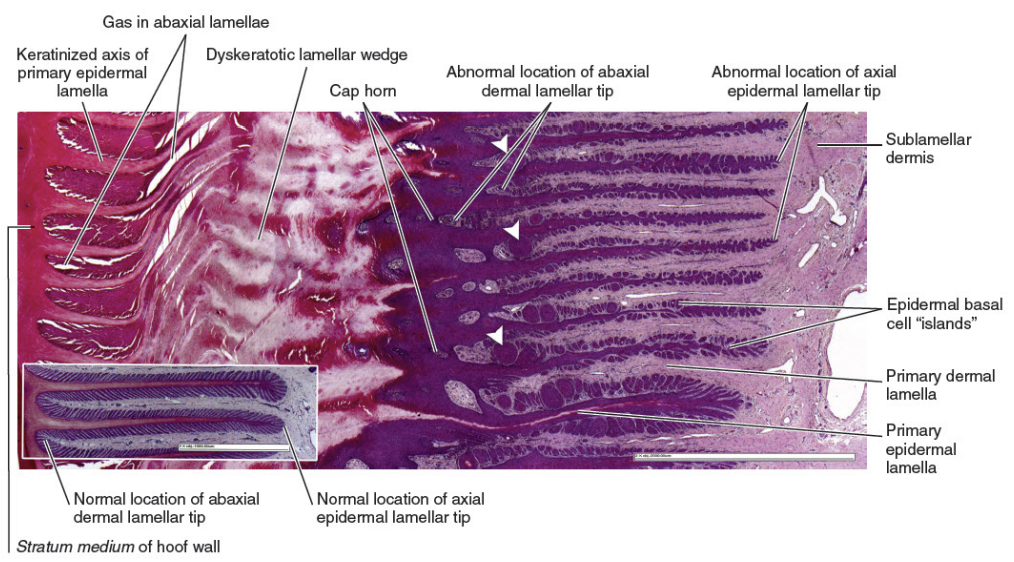 Fig 9. Chronic laminitis histopathology in an adult Standardbred gelding seven weeks after oligofructose induced laminitis (the sepsis-related laminitis model).The laminitis-affected epidermal lamellae are triple their normal length, approximately 4.3 mm longer than normal. Lamellar displacement of this magnitude is associated with dislocation of the distal phalanx and is reflected on lateromedial radiographs as an increase in the distance between the distal phalanx and the hoof wall and an increase in the “founder distance”. There is severe compromise to the suspensory apparatus of the distal phalanx (SADP) because most secondary epidermal lamellae (SELs) are no longer connected to the central keratinized axes of primary epidermal lamellae; the surface area of SADP attachment is thus significantly reduced A large mass of radiopaque dyskeratotic horn, the “lamellar wedge,” now occupies this lamellar avascular zone. The lamellae adjacent to the stratum medium of the hoof wall are empty of tissue but contain gas (possibly air) that shows as a radiolucent line on lateromedial radiographs. Copyright ‘The Illustrated Horse’s Foot’ by Christopher C. Pollitt. Elsevier. St Louis. ISBN: 9780702046551. The stretched elongated lamellae allow the distal phalanx to sink into the hoof capsule. Initially this results in a small but significant increase in distance between the outer hoof wall and the dorsal distal phalanx. This may be measurable on good quality radiographs and venograms. Early radiographs are a yardstick against which to measure 8 subsequent exacerbation. The formation of a lamellar wedge is often described as a hallmark of chronic laminitis (Figs 10 and 12). 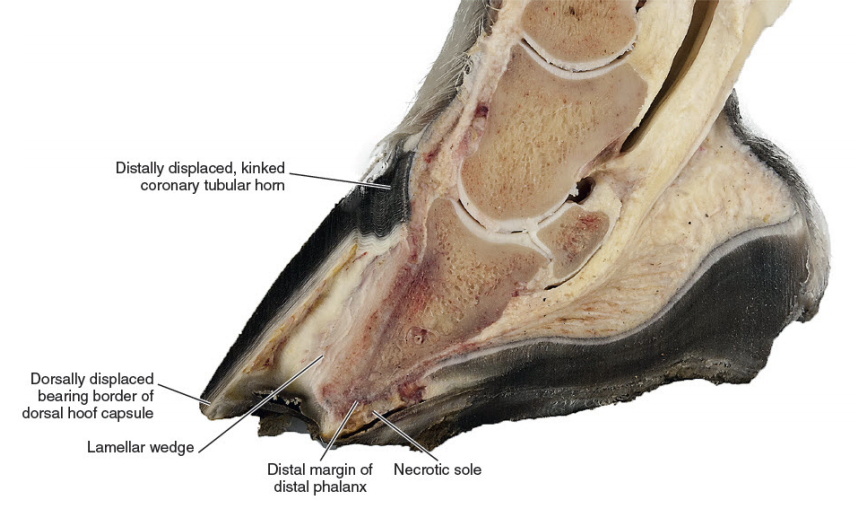 Fig 10. Pony with hyperinsulinaemic laminitis of 10 weeks duration. The distal phalanx has sunk deep into the hoof capsule, and its dorsal solear margin is in contact with the now necrotic horny sole. The founder distance is twice normal, and the coronary horn tubules are kinked and displaced distally, explaining the apparent retardation of dorsal hoof growth shown above. There is a large lamellar wedge between the dorsal hoof wall and the parietal surface of the distal phalanx. The distal part of the wedge is made up of tubular terminal horn and dorsal sole that is likely proliferating, expanding and growing palmarly in the direction of the distal margin of the distal phalanx. The bearing border of the dorsal hoof wall is distracted so far dorsally that it is unable to bear weight. This forces the foot to be loaded on the dorsal sole directly beneath the dislocated distal phalanx. This explains the bone lysis and modelling, the contused solear dermis, the pressure necrosis and infection of the sole, and the intractable pain suffered by the pony. Copyright ‘The Illustrated Horse’s Foot’ by Christopher C. Pollitt. Elsevier. St Louis. ISBN: 9780702046551. Horses with severe laminitis develop progressively greater venographic changes (especially filling deficits). Serial venography gives important information into otherwise nonvisible soft tissue pathology (Fig 11). Venographic changes occur in virtually all cases of clinical laminitis often when subtle plain radiographic changes are inconclusive. Insignificant initially, filling deficits become more complete as the weeks go by. At 7 weeks there are usually prominent deficits in the coronary band and toe venous circulations. These 9 progressively worsen until, in some cases, the entire dorsal wall appears to have no venous circulation. 16 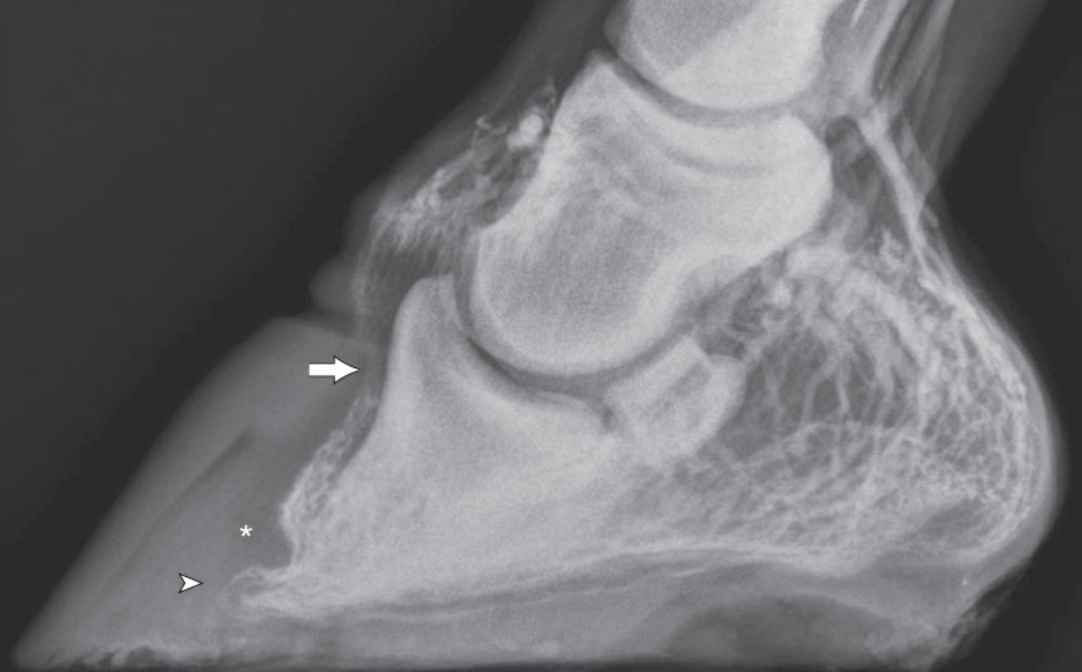 Fig 11. Thoroughbred colt front foot venogram nine months after developing colitis. The radiodense material occupying the notch in the distal phalanx is outlined by contrast medium (asterisk). The absence of contrast in the space occupying mass suggests an epidermal origin. The abnormal location and orientation of contrast-filled terminal and solar papillae (arrowhead) indicates the presence of dislocated tubular horn. The proximal hoof wall, abnormally close to the DP extensor process (arrow), is not associated with bone lysis but has compressed the veins in this region and prevented their filling with contrast. Copyright ‘The Illustrated Horse’s Foot’ by Christopher C. Pollitt. Elsevier. St Louis. ISBN: 9780702046551. When the distal tip of the distal phalanx descends into the hoof capsule it not only crushes the sole corium but drags downwards the growth zone of the dorsal sole and white line. As with the coronet this growth zone continues to proliferate but instead of the normal downwards direction it grows inwards towards the tip of the distal phalanx. Here the 10 pathological changes are more obvious. Not only are veins compressed the pressure is sufficient to lyse the tip of the distal phalanx. 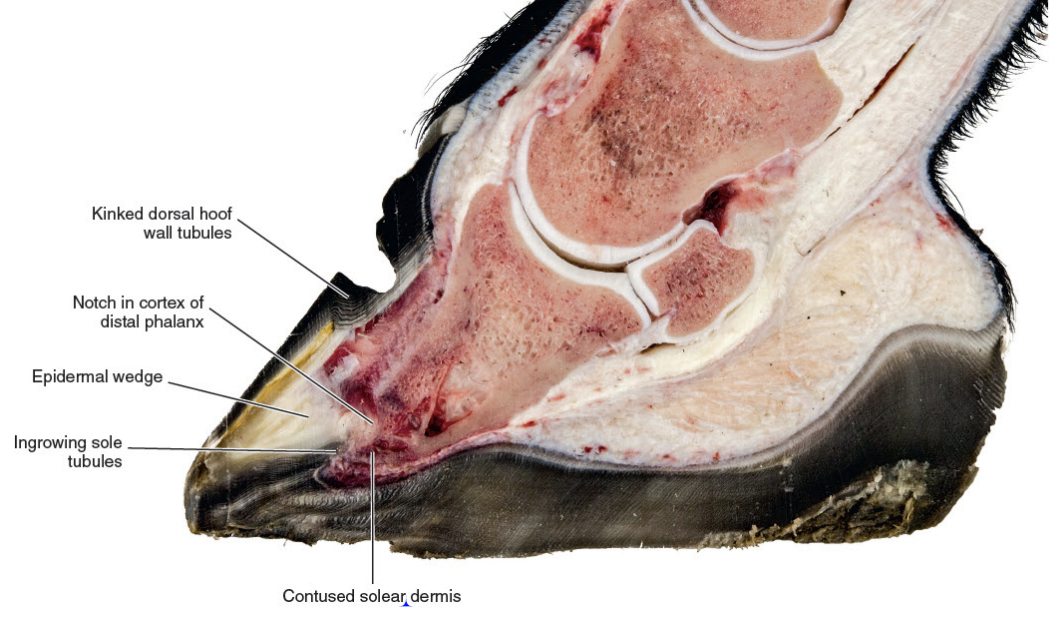 Fig 12. Thoroughbred colt front foot sagittal section nine months after developing colitis. SADP failure and sinking of the distal phalanx (DP) has occurred. The coronary dermis and coronary horn production appear normal. The dorsal hoof wall is not parallel to the parietal DP surface, indicating some rotation of the hoof capsule. The DP margin is abnormally close to the dorsal sole; the solear dermis in this region is contused. There is a lytic notch in the distal parietal cortex of the DP, just proximad to the distal margin, that is occupied by in-growing epidermal tissue. The source of the epidermal tissue is a large toe wedge consisting of dysplastic lamellae, terminal (white line), and dorsal sole tubules. The zones of hard, inward growing toe and terminal wall tubules approach the front half of the foot and may contribute to inexorable rotation of the distal phalanx; the lamellar wedge slowly pushing the tip of the bone backwards and downwards. 17 This is contrary to the widely held belief that it is the pull of the deep flexor tendon that causes distal phalanx rotation. Soft tissue and vascular compression and bone lysis is likely painful and contributes to the lameness of chronically foundered horses. If left unchecked the inward growing hoof of the proximal and distal hoof wall progressively destroys foot architecture eventually leading to incurable bone pathology. 17 Early resection of the hoof wall in a zone corresponding to the in growing coronet and toe appears to release compression of the tissues beneath and, depending on the extent of the soft tissue and bone pathology, restore a semblance of normal hoof growth. 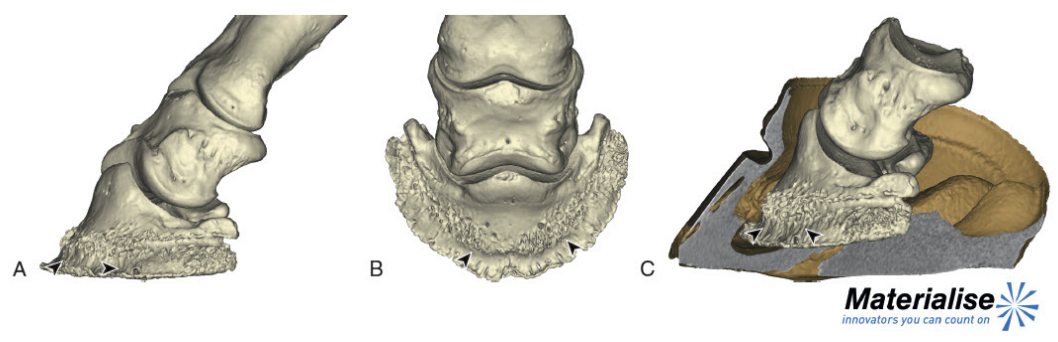 Fig 13. Mimics® models of CT data from the foot of the Thoroughbred colt with laminitis after colitis. There is extensive modeling of the distal phalanx and what appeared to be a “ski-tip” notch on lateromedial radiographs is actually a broad zone of bone lysis that has created a deep groove (arrowheads ) in the distal bone, extending over the dorsal half of the bone ( A and B ). Proximal to the notch the parietal cortex is characterized by spicules of new bone formation. The relationship between the hoof capsule and the remodeled distal phalanx is shown in C. Ridges of hard tubular horn project toward the DP groove. Copyright ‘The Illustrated Horse’s Foot’ by Christopher C. Pollitt. Elsevier. St Louis. ISBN: 9780702046551. Conclusion Thirty year of research has led to a better understanding of laminitis. With 117 laminitis/foot biology scientific publications bearing my name my co-workers and I have disseminated new knowledge to audiences around the globe. One of the roles of veterinary academics is to generate valid scientific evidence on the cause and treatment of disease. However, the work will be forgotten unless practitioners in the field recognise its potential, adapt it to clinical conditions and practice evidence based medicine. We now know that the old standby treatments such as vasodilators (acepromazine), nonsteroidal anti-inflammatory drugs (NSAIDs) and anticoagulants (heparin) have zero influence on the outcome. Whereas distal limb cooling has a potency that is not only effective but startling. Distal limb cooling to prevent and treat laminitis is currently the only scientifically validated option. Strategies to control the most common cause of laminitis, hyperinsuliaemia (HI) are beginning to appear. The incidence of HI is down and owners and care-givers are now generally aware the dynamics of pasture growth and when it can trigger foot pain. I am admittedly a ‘one disease veterinarian’ and laminitis, ‘the emperor of all foot maladies’ has fascinated me for decades – how can such a highly evolved epidermal structure like the horse’s foot suffer such devastating pathology in such a short period of time, with such agonising consequences. I have an enduring passion to see laminitis prevented if not cured and shall continue to do so. I agree with the great Einstein – ‘I have no special talent. I am only passionately curious.’ ‘Education is not the learning of facts, it’s rather the training of the mind to think.’ References 1. Pollitt CC. Basement membrane pathology: a feature of acute equine laminitis. Equine Vet J 1996;28:38-46. 2. Visser MB, Pollitt CC. The timeline of lamellar basement membrane changes during equine laminitis development. Equine Vet J 2011;43:471-477. 12 3. Underwood C, Collins SN, Mills PC, et al. Regional intravenous limb perfusion compared to systemic intravenous administration for marimastat delivery to equine lamellar tissue. J Vet Pharmacol Ther 2015;38:392-399. 4. Visser MB, Pollitt CC. The timeline of metalloprotease events during oligofructose induced equine laminitis development. Equine Vet J 2012;44:88-93. 5. Pollitt CC, Davies CT. Equine laminitis: its development coincides with increased sublamellar blood flow. Equine Vet J Supplement 1998;26:125-132. 6. Medina-Torres CE, Underwood C, Pollitt CC, et al. Microdialysis measurements of lamellar perfusion and energy metabolism during the development of laminitis in the oligofructose model. Equine Vet J 2016;48:246-252. 7. French KR, Pollitt CC. Equine laminitis: cleavage of laminin 5 associated with basement membrane dysadhesion. Equine Vet J 2004;36:242-247. 8. Pollitt CC, Daradka M. Equine laminitis basement membrane pathology: loss of type IV collagen, type VII collagen and laminin immunostaining. Equine Vet J Suppl 1998:139-144. 9. Asplin KE, Patterson-Kane JC, Sillence MN, et al. Histopathology of insulin-induced laminitis in ponies. Equine Vet J 2010;42:700-706. 10. de Laat MA, Patterson-Kane JC, Pollitt CC, et al. Histological and morphometric lesions in the pre-clinical, developmental phase of insulin-induced laminitis in Standardbred horses. Vet J 2012;195:305-312. 11. de Laat MA, van Eps AW, McGowan CM, et al. Equine Laminitis: Comparative Histopathology 48 hours after Experimental Induction with Insulin or Alimentary Oligofructose in Standardbred Horses. J Comp Pathol 2011;145:399-409. 12. Karikoski NP, Patterson-Kane JC, Asplin KE, et al. Morphological and cellular changes in secondary epidermal laminae of horses with insulin-induced laminitis. Am J Vet Res 2014;75:161- 168. 13. Galantino-Homer HL, Johnson PJ, Engiles JB, et al. Loss of lamellar epidermal cytolinker and desmosomal proteins: Does it contribute to the failure of the suspensory apparatus of the distal phalanx in equine laminitis? Journal of Equine Veterinary Science 2013;33:849-851. 14. Wang L, Pawlak EA, Johnson PJ, et al. Impact of laminitis on the canonical wnt signaling pathway in Basal epithelial cells of the equine digital laminae. PLoS ONE 2013;8:e56025. 15. van Eps AW, Pollitt CC. Equine Laminitis model: lamellar histopathology 7 days after induction with oligofructose. Equine Vet J 2009;41:735-740. 16. Baldwin GI, Pollitt CC. Progression of venographic changes after experimentally induced laminitis. Veterinary clinics of North America Equine practice 2010;26:135-140. 17. Collins SN, van Eps AW, Pollitt CC, et al. The Lamellar Wedge. Veterinary Clinics of North America-Equine Practice 2010;26:179-195. |