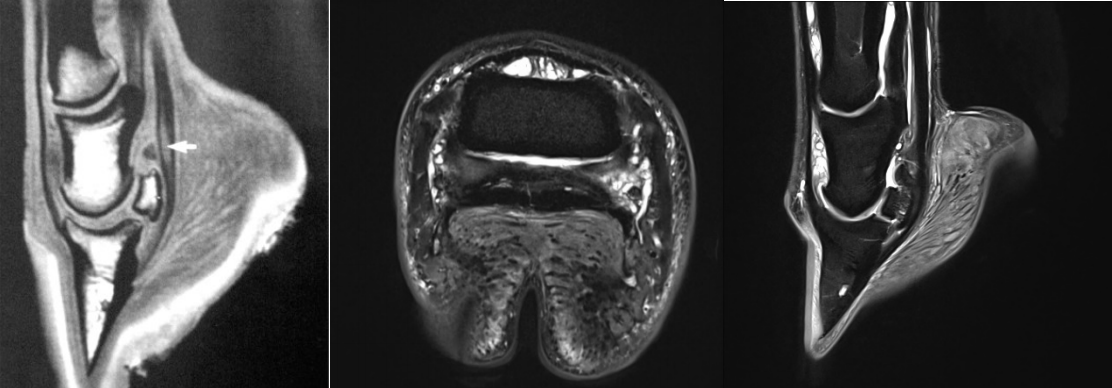
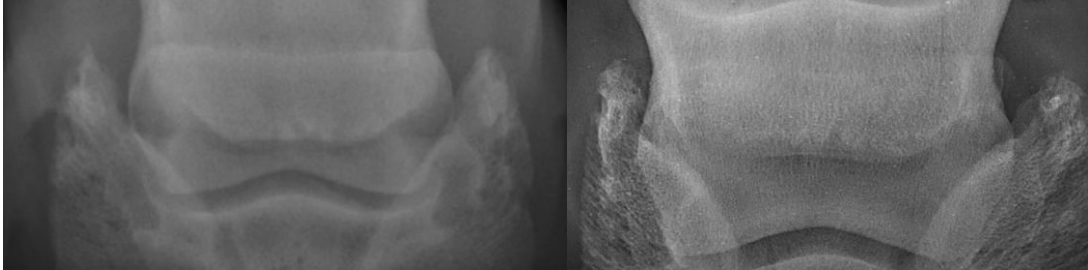
| Some thoughts on Navicular Disease… Stephen E. O’Grady, DVM 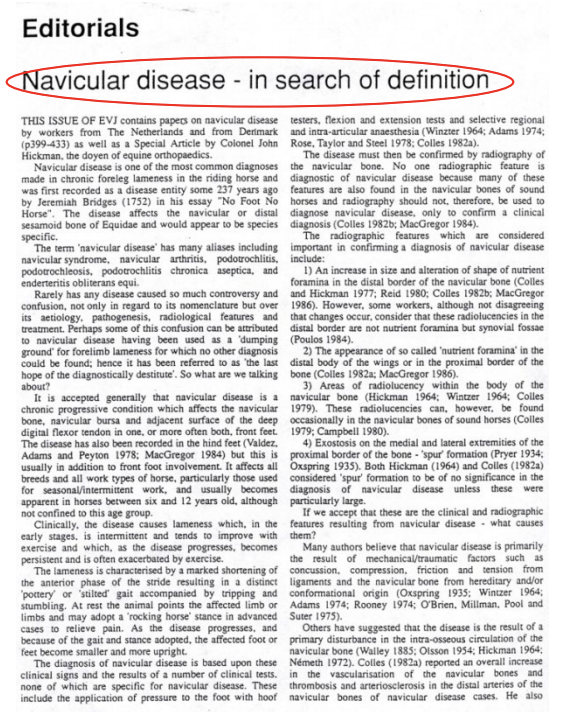 It is not uncommon even today, that if a horse presents with a bilateral forelimb lameness and blocks sound with a posterior digital (PD) nerve block, the horse is often diagnosed with navicular disease (ND). However, the incidence of true navicular disease may occur far less than previously thought. There are other names for navicular disease such as podotrochleosis, podotrochlitis, palmar foot pain and navicular syndrome. Perhaps it is splitting hairs, but navicular disease could be defined as inflammation/ degeneration of the navicular bone (possibly confirmed with radiography). Or it could be defined as podotrochlitis which is inflammation/pathology of the podotrochlear apparatus which comprises the navicular bone, bursa, suspensory ligaments, impar ligament or the DDFT lying adjacent to the bone (possibly confirmed with MRI) (Turner 2020). Historically, navicular disease was considered to be a single disease but there are probably many different clinical conditions, with different etiologies, that cause pain in the navicular apparatus. The problem with the diagnosis of navicular disease is that determining if pain is coming from the palmar portion of the foot is difficult as the palmar digital nerve (PDN) block desensitizes the entire foot (Schumacher et al EVE 2019). Therefore, as we have no nerve block that will anesthetize just the palmar section of the foot, positive results are not specific for navicular disease! The PDN block cannot differentiate between DIP joint pain, navicular apparatus pain, solar pain, or other causes of heel pain. Blocking the navicular bursa can help localize the pain but this block also desensitizes the dorsal sole and the section of the DDFT in the foot. It is not uncommon even today, that if a horse presents with a bilateral forelimb lameness and blocks sound with a posterior digital (PD) nerve block, the horse is often diagnosed with navicular disease (ND). However, the incidence of true navicular disease may occur far less than previously thought. There are other names for navicular disease such as podotrochleosis, podotrochlitis, palmar foot pain and navicular syndrome. Perhaps it is splitting hairs, but navicular disease could be defined as inflammation/ degeneration of the navicular bone (possibly confirmed with radiography). Or it could be defined as podotrochlitis which is inflammation/pathology of the podotrochlear apparatus which comprises the navicular bone, bursa, suspensory ligaments, impar ligament or the DDFT lying adjacent to the bone (possibly confirmed with MRI) (Turner 2020). Historically, navicular disease was considered to be a single disease but there are probably many different clinical conditions, with different etiologies, that cause pain in the navicular apparatus. The problem with the diagnosis of navicular disease is that determining if pain is coming from the palmar portion of the foot is difficult as the palmar digital nerve (PDN) block desensitizes the entire foot (Schumacher et al EVE 2019). Therefore, as we have no nerve block that will anesthetize just the palmar section of the foot, positive results are not specific for navicular disease! The PDN block cannot differentiate between DIP joint pain, navicular apparatus pain, solar pain, or other causes of heel pain. Blocking the navicular bursa can help localize the pain but this block also desensitizes the dorsal sole and the section of the DDFT in the foot. There is a plethora of clinical signs that can be associated with navicular disease; some or all of them may exist with the condition. ND may begin as an intermittent lameness or gradual loss of performance slowly progressing to a chronic bilateral forelimb lameness, the horse may point alternate feet or pack bedding under the feet, there may be a discrepancy in the size and shape of the feet with the narrower foot being lamer and abnormal hoof conformation (long toe low heel or sheared heels). In motion, the gait is generally short and ‘stilted’, and the horse tends to stumble. The horse will tend to land toe first (to avoid heel pain) and the lameness will be accentuated trotting in a circle on hard ground. The horse may or may not show a positive response to hoof testers or other diagnostic tests such as a flexion test which causes hyperflexion of the distal limb, a hoof extension test using a toe wedge which causes compression between the DDFT and the navicular bone or a frog wedge test which puts pressure on the navicular bursa. The diagnosis of true navicular disease is difficult and time consuming. The diagnosis should include a relevant history of a chronic bilateral forelimb lameness and several of the clinical signs described above. Furthermore, the horse should respond positively to at least two of the diagnostic tests and when possible, block sound to an intrabursal nerve block. Imaging should give confirmatory evidence that there is radiographic pathology in the bone (Figure 1) or lesions seen on MRI in the podotrochlear apparatus (Figure 2) or both.
Navicular Changes My practice does a lot of second opinions on forefoot radiographs acquired during prepurchase examinations. Obviously, these horses are considered sound and often performing at the top of their game. Frequently, in the examination/ radiographic report, the clinician will state that there are ‘changes in the navicular bone consistent with navicular disease’. But what does this mean?! Overtime, increased exercise, training, competitions, etc., will produce normal modeling of the navicular bone if the stress is kept within physiologic limits. These physiologic changes could appear as sclerosis on the ventral border, multiple inverted synovial fossa (cones) or enthesophytes at the wings of the bones (Figure 3). When considering so-called navicular bone changes, one should consider the following:
Navicular Syndrome A syndrome is defined as a collection of clinical signs and symptoms frequently appearing together or a condition characterized by a set of associated symptoms but without a known cause. When presented with a chronic forelimb lameness that improves with a PD nerve block, one will generally gravitate to the deformable structures in the palmar/ plantar section of the foot rather than the more stable dorsal section. The problem faced is, with this nonspecific nerve block, is the pain arising from the internal structures (podotrochlear apparatus), the hoof capsule or a combination of both. When the term navicular syndrome is used, it would infer that there is not a specific diagnosis but rather two symptoms. Firstly, the horse is lame and goes sound with a PD nerve block. Secondly, the imaging does not supply any pathologic finding. The author sees a multitude of horses with abnormal hoof conformation such as a long toe with low or underrun heels often combined with short shoes that are lame and diagnosed with navicular syndrome. Radiographs are inclusive and when the appropriate farriery is applied, soundness returns. In short, a definitive diagnosis of navicular disease demands a careful and thorough examination: history of lameness and competitions, inspection at rest and in motion, characterization of pain response to various stimuli, effect of diagnostic anesthesia procedures and appropriate diagnostic imaging. Additionally, it must be remembered that – within the context of a prepurchase examination - the prognostic value of diagnostic imaging in a sound and unmedicated horse is virtually non-existent. Finally, clinicians must be careful diagnosing a horse with navicular disease or navicular syndromes without convincing evidence. This diagnosis will form part of the horse’s record and will have a profound influence on a prospective purchaser if the horse is offered for sale. |