| Biomechanics as a Guide to Therapeutic Farriery Andrew H. Parks, MA, VetMB, DACVS Biomechanics provides at least two different types of information relevant to therapeutic shoeing. First, it provides information about the relationship between the distal phalanx and the hoof capsule, and the relationship between the phalanges, navicular bone, and metacarpus/metatarsus. Second, it provides diagnostic information that can identify which structure is injured and the nature of the injury. This discussion will focus on the latter. Additionally, radiography is a valuable aid for placement of a shoe in relation to the position of the distal phalanx. Every therapeutic shoe uses a few biomechanical principles:
For a review of the basic biomechanics of the equine foot…please see here.
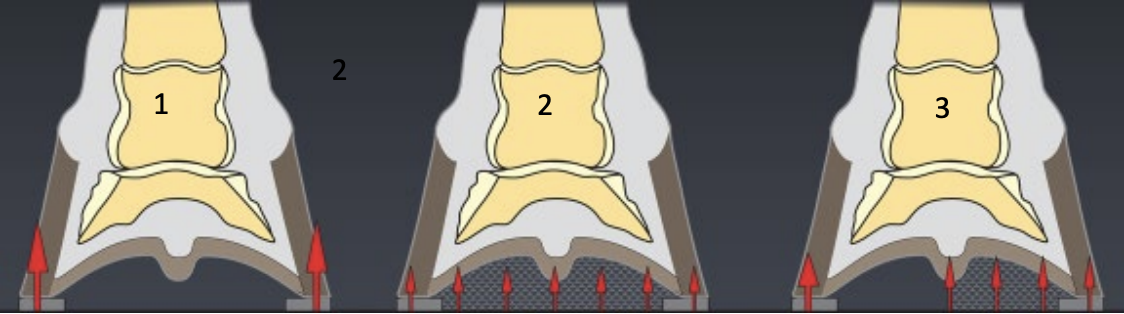
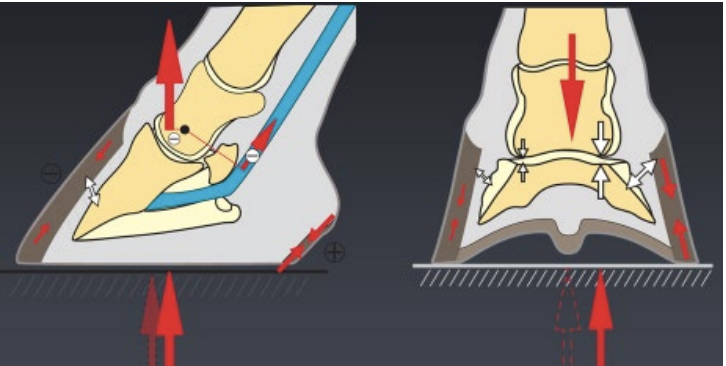
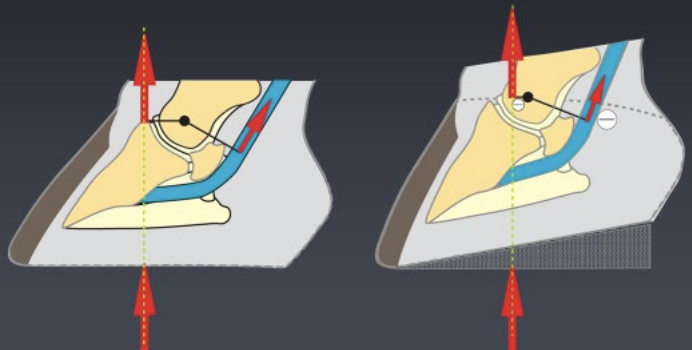
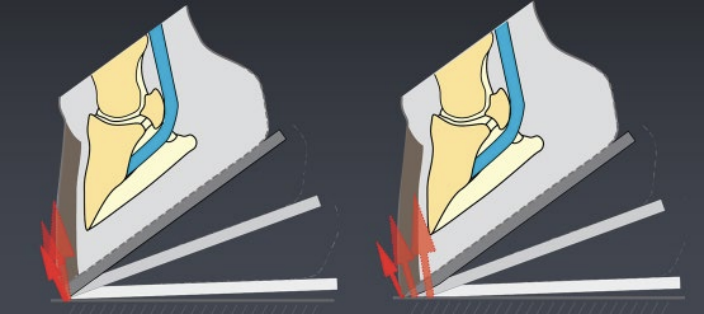
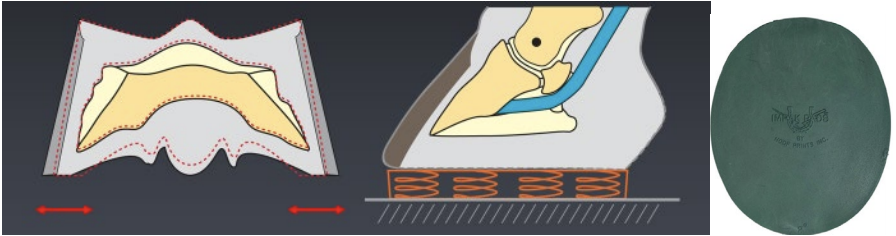
Symmetrical or asymmetrical distribution of load (weight) on the ground surface of the foot can be used to either decrease or increase pressure on any given area of the foot. For example, pour-in pads distribute the ground reaction force broadly across the ground surface of the foot whereas using a shoe with a narrow web will concentrate the ground reaction force on the distal surface of the wall. Asymmetrical distribution is used to apply pressure to a focal section on the solar surface of the foot (Figure 1A ). Asymmetrical distribution of the ground reaction force on the ground surface of the foot will cause the center of pressure to change and is likely to have a variety of effects depending on the structure (Figure 1B). For example, in the frontal plane, placing a wedge on one side of the foot will move the center of pressure towards the side that is elevated. The moments about the distal interphalangeal joint in the sagittal plane can be changed by elevating the toe or heels, a maneuver that is effective both at rest and at exercise (Figure 1C). The moments about the distal interphalangeal joint during the break over phase of the stride are affected by the position of break over on the shoe (Figure 1D). The distal interphalangeal joint exhibits limited movement in the frontal plane, so there are also moments about the joint in the frontal plane. Changing the rate of deceleration as the foot lands is primarily directed at decreasing maximum deceleration (Figure 1E), which may be achieved by incorporating a material between the foot and the shoe that compresses during impact. It should be noted that changing any one of these principles is likely to change at least one other. Additionally, it should be noted that while there are only a few biomechanical principles to follow; however, there are many ways to implement them. Determining a therapeutic shoeing strategy requires several sequential questions to be considered and addressed:
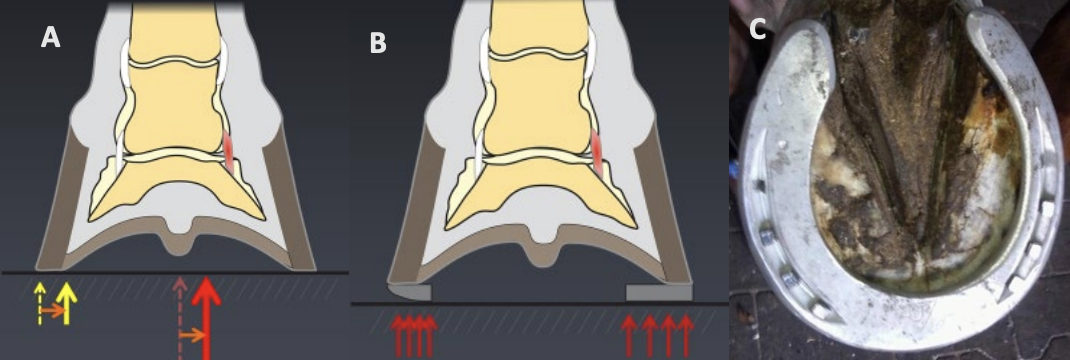
The affected tissue is identified by a combination of the physical examination, diagnostic imaging, and diagnostic analgesia. Ligaments and tendons are stressed under tension while bone and joints are primarily stressed under compression. Additionally, the lamellae are stressed under tension and the tissues of the sole are stressed under compression. The application of biomechanical principles and shoeing manipulations are best demonstrated by examples. Desmitis of the collateral ligament of the distal interphalangeal joint is not an infrequent MRI diagnosis. As a ligament, it is stressed under tension, that is anything that tends to lengthen the ligament will increase the tension in it. Therefore, the therapeutic goal is to shorten the ligament and limit how much it can be stretched. At rest this is accomplished by moving the center of pressure towards the side of the ligament which will minimize the opening of the joint on that side and thus minimize lengthening the ligament. The joint on the affected side will also tend to open and the ligament lengthen when a horse is turning away from that side. To minimize lengthening the ligament as the horse turns, the associated moment in the frontal plane can be decreased. The simplest way to move the center of pressure to the affected side if the horse is standing on a deformable surface is to make the branch of the shoe on the affected side wider than the contralateral branch. To ease movement away from the affected side, the opposite branch of the shoe is rounded (Figure 2).
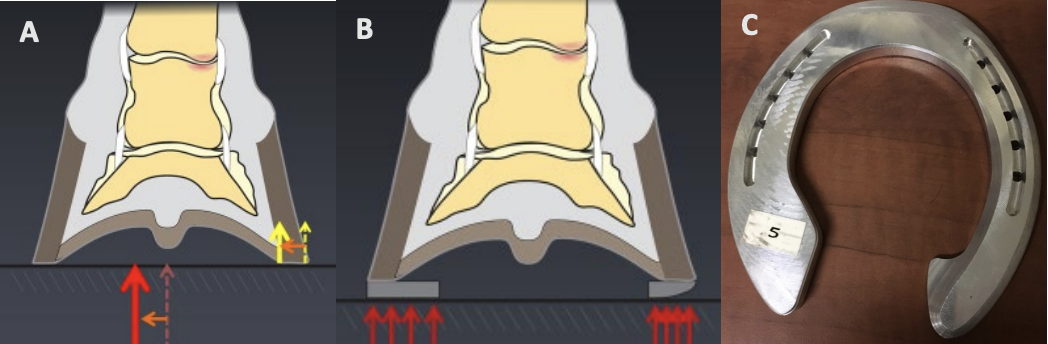
Asymmetrical bone bruising in the subchondral bone or loss of cartilage on either side of one of the interphalangeal joints that are identified on MRI should logically be treated in the opposite manner to collateral ligament injury. That is, the structures are stressed under compression and therefore, the center or pressure should be moved away from the affected side and break over eased on the affected side.
Deep digital flexor tendon injury within the foot is also a relatively common MRI diagnosis. As a tendon, decreasing its length decreases its tension (force). Therefore, the goal is to shorten the tendon when standing at rest and the stance phase of the stride and limit its tension at break over. The tendon can be shortened at rest by applying a wedge to the heels and at break over by reducing the lever arm as break over begins by moving the point of break over in a palmar direction (Figure 1C & 1D). There are several reasons why therapeutic shoeing might be ineffective or fail:
Additionally, there are occasions when an injury is present, but the severity of the disease or severity of the symptoms are sufficiently mild that the injury is likely to heal regardless. |