|
Pedal Osteitis is Not a Disease Stephen E. O’Grady, DVM
Veterinarians and farriers still struggle with the term pedal osteitis. Pedal osteitis has been labeled as a disease, a diagnosis along with a large array of treatments purported to resolve it. The term pedal osteitis may be a misnomer as osteitis is defined as inflammation of bone which may not be accurate. Pedal osteitis is no more than a radiographic description of structural changes at the solar margin of the distal phalanx rather than a proven disease and cause of lameness (Dyson 2011). The exact pathophysiologic mechanism which causes these associated radiographic changes is not clear; therefore, it is difficult to consider pedal osteitis a primary disease. There may be a variety of causes leading to the radiographic changes noted at the solar margin of the distal phalanx, thus pedal osteitis would be an inappropriate definitive diagnosis by itself (Moyer et al 1999). Adding to this dilemma, local anesthesia of the posterior digital nerve and anesthetic solution injected into the DIP joint or the navicular bursa will each anesthetize the solar surface of the foot at the toe (Schumacher et al 2019). This pattern of diagnostic anesthesia clearly illustrates that the sole/solar margins can’t be isolated to make a definitive diagnosis.
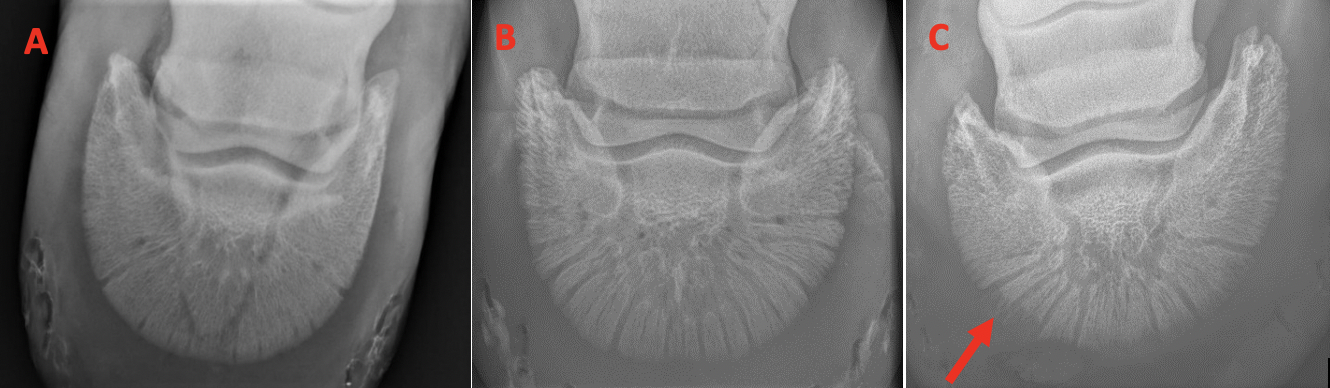
Radiographic appearance It should be stated from the onset that there are variations in the radiographic appearance of the distal phalanx in normal horses due to age, use, ground surface, foot conformation and farriery. The distal phalanx is viewed using a dorsoproximal–65-degree–palmarodistal oblique view (DP-65-PDO). Digital radiography allows the magnification and contrast of the image to be changed which provides excellent assessment of the solar border. It should also be noted that pedal osteitis is seldom observed in the hind feet as it appears to be a change associated with weight bearing in the forefeet. In a model image of the distal phalanx, the body/solar margin of the bone has uniform density throughout, the solar margin is generally regular and smooth, the radiating vascular channels are variable in number and width and may widen close to the solar margin in normal horses. Radiographic signs of pedal osteitis are characterized by a focal or generalized demineralization around the solar margin of the distal phalanx, widening of the vascular channels and an irregular solar margin border. Radiographic changes associated with pedal osteitis, once established, will tend to persist over the long term and therefore are not synonymous with active inflammation (Figure 1).
Etiology Pedal osteitis is a radiographic finding that describes demineralization and bone resorption of any aspect of the solar margin of the distal phalanx. The pathophysiologic mechanism remains speculative but appears to be inflammation/hyperemia around the margin of the bone induced by repetitive trauma. The inflammation in the active state can be verified using nuclear scintigraphy. The trauma appears to be associated with lack of protection (sole thickness/depth) on the solar surface of the foot and excess pressure exerted on the soft tissue adjacent to the margin of the bone during weight bearing. It appears that abnormal foot conformation would contribute to the onset/progression of pedal osteitis. The long toe-low heel conformation overloads the palmar section of the foot and the palmar processes will show an increased trabecular pattern, many small lucent areas along with the radiographic changes to the solar margin described above. The excessive toe length creates leverage on the dorsal section of the foot which leads to flat soles and decreased sole growth. The club foot conformation overloads the dorsal section of the foot leading to flat soles and decreased sole growth. The sheared heel conformation promotes an asymmetric landing pattern which overloads one side of the foot leading to signs of pedal osteitis on the overloaded side (Figure 1C).
Thoughts on farriery Although studies suggest the radiographic changes associated with pedal osteitis can’t be improved, the condition can be prevented and or controlled with the appropriate farriery. Good basic farriery that adheres to biomechanical principles is used to maintain/improve structures on the solar surface of the hoof capsule that afford protection to the internal structures. Attempts to improve hoof capsule distortions that overload sections of the hoof with the appropriate farriery is not only helpful but essential. Whatever farriery method used should strive to increase sole growth if possible and decrease the pressure on the sole. It should be remembered that during weight bearing, the distal phalanx descends within the hoof capsule further increasing the load on the soft tissue One farriery method I see used frequently to address thin soles is a pour-in pad applied over the solar surface between the branches of the shoe. The biomechanical principle of the pour-in pad is to increase the ground surface of the foot and redistribute the load placed on the solar surface of the foot. However, its use on a foot with a thin sole may be questionable as the increased pressure on the sole appears to inhibit any additional sole growth and over time with continued use, will further decrease the thickness of the sole.
Summary Since the term pedal osteitis is a descriptive term rather than a definitive diagnosis, it seems appropriate that the term should disappear from the list of diseases that affect the horse’s foot or be modified to accurately describe the problem. The inherent problem in using this term is that it implies the presence of a known disease, which indicates that some knowledge exists as has how to treat with the problem. Perhaps, since this information does not exist, the radiographic changes associated with so-called pedal osteitis should just be described as "focal or generalized" loss of solar bone margins and widening of the vascular channels because of a 'known' or 'unknown' cause. Be safe. |