A fresh look at white line diseaseReprinted with permission from Equine Veterinary Education (EVE). Original published in Equine Veterinary Education Vol 23 Oct 2011.S. E. O'Grady Keywords: horse; white line disease; hoof wall separation; resection; therapeutic farriery
Summary White line disease occurs secondary to a hoof wall separation. Clinical signs may vary from not being lame to severe lameness with rotation of the distal phalanx depending on the extent of the disease affecting the inner hoof wall. The author has found that removal of the hoof wall overlying the diseased area combined with the appropriate farriery is the most important aspect of therapy.
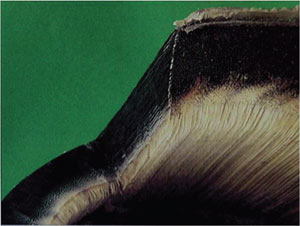
Introduction White line disease (WLD) is a disorder localised to the equine foot. The problem is widespread, the aetiology and mechanism of the disease are poorly understood and treatment is often controversial. White line disease is a term used to describe a keratinolytic process that originates on the solar surface of the hoof characterised by a progressive separation of the inner zone of the hoof wall (O'Grady 2001,2006; Moyer 2003; Pleasant and O'Grady 2009). The separation occurs in the nonpigmented horn at the junction between the stratum medium and stratum internum (Fig 1).The destruction that occurs in the separation as a consequence of WLD remains superficial to the stratum internum and does not invade the dermis. A separation in the hoof wall is considered to be a delaminating process potentially thought to originate from genetic factors, mechanical stress, inappropriate farriery and environmental conditions affecting the inner hoof wall attachment (Moyer 2003). The separation, which can originate at the toe, the quarter and/or heel, appears to be invaded by opportunistic bacteria/fungi leading to a type of infection where the organisms digest the horn allowing the separation to progress to varying heights and configurations proximally toward the coronet. The disease has been termed seedy toe, hoof wall disease, yeast infection, Candida and onychomycosis.Onychomycosis is a mycotic disease that originates in the nail bed of man and the dog. By contrast, in WLD the infection appears to have originated at the solar surface of the hoof and migrates proximally, approaching the coronet but never invading it. Keratinophilic fungi are often isolated from separated areas of the hoof wall; however, in many cases of WLD, the pathogens cultured are purely bacterial or a mixture of bacterial and fungal organisms(Turner 1998). Therefore, until proven otherwise, onychomycosis may not be the appropriate term when referring to white line disease in the horse (O'Grady 2006).
Anatomy of the hoof wall The hoof wall consists of 3 layers which are the:
The stratum externum arises from the perioplic epidermis and forms the thin outer layer of keratinised cells that give the wall its smooth glossy appearance. The stratum medium, which arises from the coronary epidermis, forms the bulk of the hoof wall and is the densest part of the horny wall. It consists of cornified epidermal cells arranged in parallel horny tubules surrounded by intertubular horn, which grow distally from the coronary groove to the basal border. In all hooves the stratum medium is always nonpigmented in the deepest inner layer(Fig 2). The stratum internum arises from the lamellar epidermis, is nonpigmented and, when combined with the dermal lamellae, is responsible for attaching the hoof wall to the distal phalanx. Distally at the sole wall junction, the dermal lamellae end in terminal papillae. These terminal papillae are lined by a germinal epidermis which generates keratinised epidermal cells which fills the space between the nonpigmented horny laminae as they grow toward the ground surface (Pollitt 2010). This association forms the bond between the hoof wall and sole known as the white line or zone (Parks 2003). When observed from the solar surface, this white line or zona alba is actually yellow in colour and has a plastic consistency when compared to the dorsal hoof wall. Aetiology The aetiology of WLD remains undetermined. The problem has been described in horses worldwide. WLD can affect a horse of any age, sex or breed. One or multiple hoofs maybe involved and affected hooves can be barefoot or shod. One or multiple horses on the same farm may be affected. It is generally agreed that WLD is a multifactorial condition that develops secondary to an initial separation or hoof wall defect (O'Grady 2006; Pleasant and O'Grady2009). It must be remembered that multiple causes for white line disease have been proposed but none have been scientifically proven. Moisture may play a role as WLD is seen more in wet humid areas, but it is also seen in hot arid conditions.Excessive moisture may soften the foot, allowing easier entry of dirt and debris into an existing separation.Continual bathing of competition horses, especially during the warmer months, may contribute to the incidence of WLD in this population of horses. Excessively dry hooves on the other hand may form cracks or separations in the hoof wall, allowing pathogens to invade. Poor hygiene has been blamed but this is questionable since WLD often appears in well managed stables. Keratinopathogenic fungi and bacteria are commonly isolated from the hoof wall defects of horses with WLD,particularly those with more extensive lesions. It is generally believed that these microorganisms are opportunistic,secondary invaders that enter the hoof wall through a separation or compromised area and then exacerbate hoof wall separation by the production of proteases that degrade keratin. Farms that experience a large number of cases of white line disease may have predisposing environmental or management conditions and/ora ubiquitous population of keratinopathogenic microorganisms (Pleasant and O'Grady 2009). The fact that WLD can be resolved with debridement alone further detracts from infection as a primary cause (O'Grady 2006;Pleasant and O'Grady 2009). Mechanical stress placed on the inner hoof wall from less than ideal hoof conformation may encourage a separation. Types of abnormal hoof conformation would include excessive toe length, long toe-low heel, club feet or sheared heels. Separation at the stratum medium/stratum internum junction of the inner hoof wall increases the stress in the intact stratum medium/stratum internum junction of the adjacent wall. Weightbearing coupled with the force of the deep digital flexor tendon becomes cyclic and will increase the distractive forces placed on this area further weakening the bond (Turner 1998). Routine hoof care is important because when feet are left unattended,dirt and debris packs into a hoof defect or separation and may result in progressive mechanical separation of the hoof wall. Vascular damage to the dermal lamellae associated with chronic laminitis results in a compromised bond between the epidermal and dermal lamellae and a loss of integrity (separation) dorsal to the sole/wall junction. White line disease can also be noted to be a sequel to tracts created by extensive subsolar or submural abscesses. Clinical signs White line disease is a threat to the soundness of the horse if damage is extensive enough to allow mechanical loss of the attachment between the stratum medium and epidermal lamellae, resulting in displacement of the distal phalanx in a distal direction (rotation). Most commonly, WLD is noted as an incidental hoof wall separation found by the farrier during routine hoof care. In the early stages of white line disease, the only noticeable changes on the solar surface of the foot maybe a widening of the sole/wall junction and small powdery areas located just in front of this junction. The change may remain focal or it may progress to involve a larger area of the hoof wall. Other early warning signs of white line disease may be thin, tender soles as noted with hoof testers, occasional heat in the feet, and the sole will become increasingly flat. If separation becomes more extensive and involves the toe and a quarter, a concavity ('dish') may be seen forming along one side of the hoof and a bulge will be present on the contralateral side directly above the affected area at the coronary band. The distal phalanx is suspended circumferentially within the hoof capsule in the state of equilibrium. When a substantial separation affecting the epidermal lamellae is present and the laminar attachment is compromised, the equilibrium is disrupted and the distal phalanx will shift toward the separation causing a concavity in the hoof wall on the opposing side of the foot thus explaining the change in the hoof wall shape. White line disease often goes undetected until the horse begins to show signs of lameness.
Diagnosis Lameness may not be observed in the early stages of the disease. Hoof tester examination does not always elicit a response. The clinical signs along with a thorough examination of the solar surface of the hoof will confirm the diagnosis. On the solar surface of the hoof, the sole/wall junction (white line) will be wider, softer and have a chalky or waxy texture. Exploring the inner hoof wall, which lies dorsal to the sole/wall junction, will generally reveal a separation filled with white/grey powdery horn material.Further exploration with a blunt probe will give the depth and extent of the cavitation (Fig 3). There may be a black serous drainage from the separation. A hollow sound will be noted when the outer hoof wall over the separation is percussed with a hammer. If lameness is present, a thorough lameness examination should be performed including diagnostic analgesia to localise and confirm the suspected area followed by radiographs. With extensive hoof wall damage, WLD accompanied by pain can mimic laminitis both clinically and radiographically.
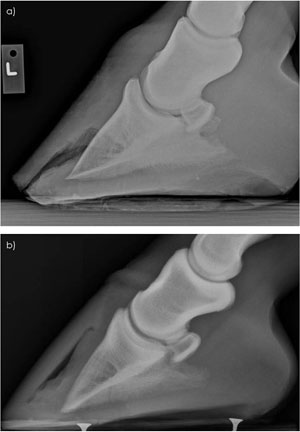
Radiographs Radiology can be very informative and should be considered necessary. Radiographs will show the extent of the hoof wall separation and whether displacement of the distal phalanx within the hoof capsule has occurred.Radiographs allow the clinician to differentiate between white line disease and laminitis (Figs 4a and b).Radiographically, the separation in the epidermal lamellae will originate at the ground surface of the foot and extend dorsally in white line disease, whereas in laminitis, the lucency will originate in the dermal lamellae and extend distally to the terminal laminar papillae. Pedalosteitis may be noted in some chronic cases of white line disease. Finally, radiographs can be used as a guide for applying the appropriate farriery treatments. Laboratory investigations Laboratory findings have been unrewarding and exert minimal influence with regards to treating this disease.Cultures are of little value since the samples taken from the separations are contaminated with dirt and multiple opportunistic organisms. Aerobic cultures usually reveal a mixed bacterial flora while anaerobic cultures are generally negative (Turner 1998). Fungal cultures require a special media and time. The most common fungal species cultured are Pseudoallsheria, Scopulariopsis and Aspergillus. A biopsy taken at the junction between the normal and affected hoof wall shows a mixed population of microorganisms. These will generally include coccobacilli, yeast organisms and fungal spores.Inflammation in the laminar dermis will be seen deep to the affected area (Turner 1998). Treatment Farriery Improving hoof conformation and correcting any hoof capsule distortion that may have contributed to the hoof wall separation is essential. If left untreated, WLD will allow the separations to become extensive and displacement of the distal phalanx is a likely sequel. In order to prevent small lesions from becoming extensive, farriers are encouraged to examine each foot carefully during routine trimming. Abnormal areas or separations involving the inner hoof wall should be explored and debrided down to solid horn whenever possible. Ignoring or incompletely debriding early lesions is likely to lead to progression of the separation. Any cavity that is left after debridement should be filled with a medicated hoof putty (Keratex)1 before being covered with a shoe. Treatment of white line disease is directed toward protecting and unloading the damaged section of the foot with therapeutic shoeing combined with resection of the hoof capsule overlying the affected area. As a resection disrupts the continuity and weightbearing strength of the hoof wall, some type of shoe should be applied for protection, to stabilise the hoof capsule and to prevent the horse from utilising the sole for weightbearing. If the separated area of the foot is determined to be extensive, it is important to plan and perform the farriery prior to the outer hoof wall being resected. The type of shoe used and the method of attachment depend on the extent of the damaged hoof wall. If the defect is small, the hoof can be shod with an open shoe paying strict attention to any abnormal hoof conformation. If the defect is large and the overlying segment of hoof wall needs to be resected, some type of bar shoe is indicated to stabilise the hoof capsule. If the separation at the toe and often a quarter become extensive, it is useful to redistribute the weight to the palmar/plantar section of the foot and also move the breakover in a palmar/plantar direction. A line is drawn across the widest part of the foot and the foot trimmed from this line palmarly/plantarly in a tapered fashion. Any excessive toe length is reduced from the dorsal hoof wall using a rasp. This method of trimming will create 2 planes on the solar surface of the foot and thus unload the toe. The shoe is fitted so breakover is placed just dorsal to the margin of the distal phalanx in an attempt to remove the 'lever arm' effect at the toe. This will also stop the 'pinching' effect that often occurs at the junction of normal hoof wall and the resection.
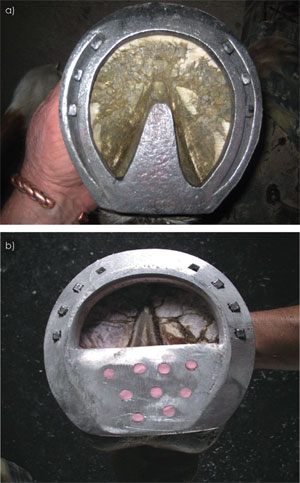
If the resection is to be extensive and/or if rotation of the distal phalanx is present, the foot should be trimmed according to the radiographs and some form of bar shoe(heart bar) or shoe with a heel plate should be used. This type of shoe allows some weightbearing to be transferred from the hoof wall to the frog (heart bar) or frog, sole and bars (heel plate) (Figs 5a and b). Alternatively, the foot may be shod with an open shoe and the solar surface of the foot between the branches of the shoe is filled with some type of silastic material. If there is limited hoof wall available in which to place nails or shoes cannot be nailed on safely, glue-on shoes may be used. The author attaches an aluminum shoe directly to healthy horn on the ground surface of the foot and the outer hoof wall at the heels using an acrylic composite (Equilox)2, thus leaving the resected area open to be observed, cleaned and debrided regularly (O'Grady and Watson 1999). In severe WLD cases where there is marked rotation of the distal phalanx, the author has been successful using a wooden shoe (O'Grady and Steward 2009). Foot casts and various types of boots have become popular in treating WLD especially after a resection has been performed but, in the author's opinion, should be avoided as casts tend to cover the affected section of the foot and boots create a continuous moist environment. Foot casts and boots should not be used as a substitute for skilled farriery as this author has not encountered a case of WLD where a shoe of some form could not be attached to the foot.
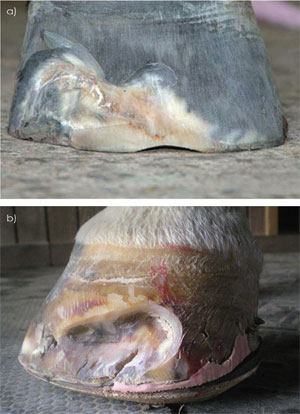
Resection Complete hoof wall resection (removal of outer hoof wall to expose diseased horn) and debridement of all tracts and fissures in the affected area is necessary. This can be readily accomplished using a loop hoof knife and half-round hoof nippers. The debridement should be continued proximally and marginally until there is a solid attachment between the hoof wall and external lamellae (Fig 6). Hemorrhage should not be encountered by the veterinarian or farrier if the debridement is performed properly. Medical or topical treatment in any form is of no value without resection of the affected hoof wall in the author's opinion. A plethora of topical medications have been described for treatment following hoof wall resection but there have been no controlled studies on any product and none in the author's opinion have been proven effective.Disinfectants/astringents such as methiolate or 2% iodine are commonly used but may have the most benefit as a dye marker to outline the remaining tracts in the stratuminternum (Fig 7). The dye marker will serve as an aid in making the remaining tracts more visible at subsequent examinations and as a guideline during debridement. Either preparation should not be applied more than weekly so as not to make the exposed lamina excessively hard and brittle. After thorough hoof wall resection, the affected area can be left open to grow out with debridement at frequent intervals. A wire brush is used daily to keep the resected area clean. Thorough exploration and debridement of any remaining tracts should take place at 2 week intervals.When the resection has grown out, a thorough examination of the sole wall junction is imperative at reshoeing intervals every 4-5 weeks. Acrylic repair of the resected area should be avoided if possible. It should only be considered in selected cases where the client is unable to treat the resected area and where cosmetics are a necessity. The composite may hide and/or foster infection and it tends to weaken the surrounding solid hoof wall, all of which can encourage reinfection. Combining an antibiotic with the acrylic has been described but has not proved to be consistently effective in the long term (Turner and Anderson 1996). If repair is performed, there should be an interface such as clay or some type of foam inserted between the acrylic composite and surface of the resection. Aftercare A change in environment is important. The feet should be kept as dry as possible throughout the recovery period.Sawdust or wood shavings appear to dehydrate the feet making them the bedding of choice and bedding should always be kept clean and dry. Limited turnout in rain or wet weather is helpful. Turnout can be delayed in the morning until the sun has dried the dew from the pasture. Commitment from the owner with regards to a continuous treatment schedule is necessary until all signs of disease have been eliminated and then the foot/feet must be monitored monthly until the hoof wall grows out. The extent of the damage will determine the approximate amount of time required to complete the treatment process. However, it is not always necessary for the horse to be out of work for this treatment period. The amount of exercise permissible while treating WLD is contingent on the extent of the damage and presence of sufficient hoof wall necessary for weightbearing. Prevention Prevention of WLD is difficult because the exact cause is unknown. Discussing the problem with the farrier and having him/her examine each foot when the horse is shod is extremely important. Any small abnormal area involving the sole/wall junction should be noted, explored and debrided down to solid horn. Proper physiological trimming and shoeing is essential for creating a strong sole/wall junction that may prevent separations and offer protection (O'Grady and Poupard 2003). Equally important is the necessity to carefully monitor horses that have previously had white line disease as it may suddenly reappear in some horses with strong hoof walls that show no previous signs of a hoof wall separation. Discussion White line disease involves the inner, nonpigmented section of the stratum medium of the hoof wall, not the sole-wall junction (zona alba, or 'white line'). Thus, 'white line disease' is somewhat of a misnomer. Nevertheless, it has become the accepted term used by the majority of farriers and veterinarians. Certainly it is a more useful term than onychomycosis, as it does not limit the primary aetiological organism to a fungal agent. Treating WLD has created a dilemma for owners,veterinarians and farriers. Owners have been deluged with many different proposed causes of WLD and a variety of treatment protocols. Numerous commercially available preparations have been marketed for treating WLD, all claiming success. The internet describes a multitude of products and methods guaranteed to provide miraculous improvement. At present, there is no convincing scientific evidence as to the efficacy of any given product.Veterinarians are often unaware of the magnitude of this problem as they only see the severe cases that present for lameness evaluation and/or when radiographic changes become apparent. White line disease may be a subtle contributor to other causes of lameness within the foot.Farriers are very aware of this disease as they are often confronted with nailing a shoe on limited or compromised hoof wall and keeping the shoe on between resets. They continually search for topical treatments since owners are reluctant to have resections performed and farriers are often reluctant to recommend resections that can be a daunting procedure. Following a hoof wall resection,farriers have traditionally performed a composite repair,often to appease the horse owner or allow the horse to continue performing. This practice should be discouraged as it prevents careful monitoring of the resection, appears to harbour organisms under the repair and may impede resolution of the disease (Pleasant and O'Grady 2009).Research, owner education and continued farrier awareness of WLD appears to be the most promising direction for the future. Author's declaration of interests No conflicts of interest have been declared. Manufacturers' addresses
References
|