Equine Foot Surgery: A Joint Venture With the FarrierReprinted with permission from the American Association of Equine Practitioners. Originally printed in the 2010 AAEP Convention proceedingsClifford M. Honnas, DVM, Diplomate ACVS; and Don Sustaire, CJF Authors' addresses: Texas Equine Hospital, 13688 S. State Highway 6, Bryan, Texas 77807 (Honnas); and 13121 Hopes Creek Road, College Station, Texas 77845 (Sustaire). © 2010 AAEP.
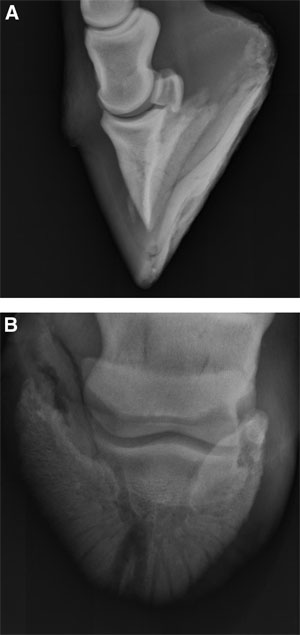
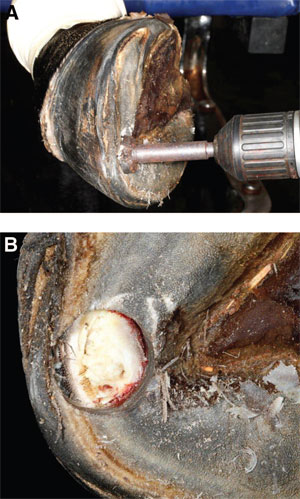
1. Introduction Surgical invasion of the horny hoof capsule is often required to access lesions caused by infection, benign tumors, and penetrating injuries. Healing of surgical defects in the hoof wall or sole is often protracted and necessitates some form of protection during the postoperative period to improve patient comfort and to decrease environmental contamination of the surgical site. Many of these surgical conditions require a team approach between the veterinarian and the farrier to achieve optimal results.This paper will discuss a variety of foot conditions for which surgery is required to attempt resolution and will also discuss farriery as an important component of postoperative care. 2. Sequestrum Removal From the Distal Phalanx The formation of a bone sequestrum involving the distal phalanx generally occurs as a consequence of the introduction of environmental pathogens into the soft tissues of the foot. Routine, long-standing foot abscesses that fail to drain to the exterior of the hoof may on occasion result in the septic process secondarily invading the adjacent bone. As the infection becomes established in the adjacent portion of the distal phalanx, the bone may lose its blood supply, resulting in development of a sequestrum.1Similarly, foreign bodies that penetrate the sole may impact the distal phalanx, causing a focal loss of blood supply and formation of a sequestrum. In addition, blood supply alterations associated with laminitis may result in sequestrum formation.1 The clinical signs that alert a practitioner or farrier to the possibility of a distal phalanx sequestrum include a history of chronic lameness, recurrent purulent drainage from the sole, and the presence of a draining tract that leads to bone. Radiographic evidence of osteolysis or sequestration of a bone segment is definitive for this condition (Fig.1). Occasionally, a sequestrum is not identified,but rather osteolysis that is evidenced by loss of normal bone density. Either of these radiographic presentations (osteolysis or sequestrum) is evidence that surgery is indicated. The infection generally affects the soft tissues of the sole, laminae, and hoof wall as well as the distal phalanx.1 Treatment is aimed at surgical debridement of the affected bone and surrounding soft tissues. The goals of surgery are to provide drainage of purulent exudates, debride infected soft tissue, and remove devitalized bone. Surgery can be performed with the horse anesthetized or standing. The senior author typically debrides the distal phalanx with the horse standing and sedated with the foot blocked. A tourniquet applied around the fetlock to compress the digital vessels against the proximal sesamoid bones will greatly facilitate visualization during surgery (Fig.2). The cornified sole surrounding the draining tract can be removed with a hoof knife, motorized burr, or, in some instances, a scalpel.1 Currently,the senior author prefers to use a Forstner drill bit on a cordless drill for penetration of the sole or wall overlying the sequestrum. This drill bit has a small center point for starting the hole and drills a flat bottom hole (Fig. 3). It allows penetration of the wall or sole without drilling into the sensitive laminae. Once the sole or wall has been penetrated,the laminae between the cornified sole and distal phalanx is removed by sharp dissection with a scalpel or sharp curette and the draining tract followed to bone. Infected bone is softer than normal bone, which is removed with a large basket spoon curette. The soft tissue and bone are curetted to healthy margins (Fig. 4).1 Postoperative care involves packing the surgical site loosely with sponges and bandaging the foot. A simple but effective bandage is made by placing a baby diaper on the bottom of the foot and securing it around the pastern with the self-stick tabs. The diaper is covered with cohesive tape,b and the cohesive tape is covered with strips of duct tape to prevent the bandage from wearing through to expose the sole. This type of bandage will generally last2-3 days or more in stalled horses.1 The surgical site is inspected at 24- to 48-h intervals,and any questionable tissue is debrided. Systemic antibiotics are indicated in many cases;however, many horses recover without antibiotics.Non-steroidal anti-inflammatories (e.g., phenylbutazone,2.2-4.4 mg/kg, q 12 h) are indicated to minimize inflammation and encourage weight bearing.1Application of a treatment plate either preoperatively or postoperatively is helpful to improve patient comfort and to simplify postoperative care (Fig.5). In most cases, healing is usually complete in8-12 wk. Once the sole has cornified, use of the treatment plate can be discontinued and a regular shoe applied. Affected horses have an excellent prognosis for return to athletic function unless laminitis is the underlying cause of the distal phalangeal infection.1 3. Keratomas A keratoma is a benign, keratin-containing soft tissue mass that develops between the hoof wall and distal phalanx.2 The occurrence of a keratoma at the sole has also been reported; however, this location is uncommon.3 The etiology of keratoma formation is unknown but may be a response to chronic irritation.2 The clinical signs are those of a progressively developing lameness that becomes more pronounced as the keratoma gradually enlarges and creates pressure between the hoof wall and distal phalanx.The lameness may be intermittent. As the keratoma enlarges, disruption of the external hoof architecture may become apparent as evidenced by a bulge in the hoof wall or inward deviation of white line.1 The diagnosis is definitively confirmed when radiography of the foot shows a semicircular or circular radiolucent defect at the margin of the distal phalanx.This radiographic lesion is the result of the expanding keratoma causing focal bone resorption.The bone margin surrounding keratoma is smooth and not sclerotic, which differentriates a keratoma from infection.1 Surgery is indicated when the lameness is confirmed to originate in the foot with diagnostic blocks,and the characteristic radiographic lesion is identified.The keratoma is approached by resecting the hoof capsule overlying the mass. The most difficult aspect of surgery is targeting the precise location to enter the hoof wall if deformities in the hoof wall do not delineate the location. This is best accomplished by taping radiopaque markers to the hoof wall and obtaining sequential radiographs to ascertain the location. A cordless drill and Forstner bit are used to remove the hoof wall overlying the keratoma.This method is less invasive than the hoof wall resection technique previously used, and both preserve the stability of the hoof wall during the convalescent period.1 Surgery can be performed in the anesthetized horse or standing using local anesthesia. The senior author prefers the standing approach for most horses unless their temperament precludes this choice. Again, a tourniquet at the level of the fetlock is used to reduce hemorrhage and aid visualization.1 Postoperatively, a foot bandage is applied and changed at 3- to 4-day intervals until the surgical defect in the hoof wall has cornified. Once granulation tissue has covered the exposed bone, astringents such as merthiolate (thiamersol) or iodine (2-7%) are applied to dry the tissue and enhance cornification. Phenylbutazone is administered as needed in the postoperative period. Antibiotics are generally unnecessary because infection does not typically accompany the keratoma.1 The prognosis for resolution of lameness and return to intended use is excellent. The hoof wall entry site usually grows down in 6-12 mo, resulting in a normal-appearing foot.1 4. Necrosis of the Collateral Cartilage Infection and necrosis of a collateral cartilage can be seen as a sequelae to lacerations, foot abscesses,puncture wounds, gravel (chronic ascending infection under hoof wall), hoof cracks, and blunt trauma(over reach injuries, kicking inanimate objects), resulting in avascular necrosis.1 Affected horses become lame as abscesses form within the cartilage. The lameness is often intermittent, ranging from mild when the abscesses are draining to the exterior to severe when the draining tracts seal for a period of time. As the infection becomes established, marked soft tissue swelling over the affected cartilage becomes apparent. Purulent drainage from the cartilage may or may not be present at the initial examination, depending on the patency of the draining tract.1 The diagnosis is made by observation of draining tracts proximal to the coronary band over the affected cartilage, or in some cases, marked swelling of the cartilage accompanied by severe lameness without accompanying drainage. Radiographs obtained with a flexible metal probe in the tract or after infusion of contrast media into the tract will help determine the depth of the tract and confirm involvement of the cartilage. Importantly, if the abscesses within the cartilage are draining at presentation, the horse may not be very lame. This should not delay surgery because lameness will recur when the draining tracts seal again. Because the cartilage is relatively avascular, antibiotics and infusion of caustic agents into the draining tracts are usually ineffective in resolving the infection.1 Colonizing the draining tracts with medical grade maggotsc (maggot debridement therapy) is one treatment option that may have merit. The idea is that the maggots will eat necrotic tissue and thereby preclude the necessity of surgery if successful.The authors do not have any personal experience with this treatment option. Surgery is indicated based on the presence of a swollen cartilage with draining tracts. Severe swelling accompanied by severe lameness in the absence of drainage would warrant an ultrasound evaluation of the cartilage and consideration of surgical exploration. Treatment is aimed at excision of the affected portions of cartilage and overlying soft tissue and establishing ventral drainage. The surgery is accomplished with the horse in lateral recumbency. As with other foot procedures, a tourniquet is applied at the level of the fetlock to enhance visualization during surgery. In addition,regional perfusion of the distal limb with antibiotics can be performed while the tourniquet is in place.Only the infected portions of the collateral cartilage need to be excised. During the surgical procedure,the foot is extended in an attempt to tense the palmar pouch of the distal interphalangeal joint and retract it from the deeper areas of dissection. The senior author prefers to access the proximal portion of cartilage above the coronary band through a curved incision based proximally. This technique preserves skin for primary closure and allows easier access to portions of the cartilage that will be accessed through the hoof wall later in the procedure.The skin flap is reflected proximally, and all accessible diseased proximal cartilage is removed. Diseased cartilage beneath and distal to coronary band is accessed and removed through a hole drilled in the hoof wall. The tissue and cartilage between the trephine hole and proximal incision is removed by sharp dissection to allow ventral drainage. If the diseased tissue extends axially toward the joint, the integrity of the joint can be assessed via arthrocentesis and distention of distal interphalangeal joint at a site remote from the surgical incision. At the completion of surgery, the skin incision is sutured,and the trephine hole is packed loosely with gauze sponges. The foot is bandaged until the skin incision is healed and the hole in the hoof wall is cornified.Systemic antibiotics are generally indicated for 7-10 days. Additionally, regional perfusion of the distal limb should be considered in cases where diseased tissue extends down to the region of the distal interphalangeal joint in a location that would risk penetration of the joint capsule with overzealous debridement.1 Considerations for the farrier include patching the hoof wall once the surgical entry site has cornified completely. Care should be taken to ensure the patch does not provide an environment to trap bacteria and induce the development of an abscess beneath the repair. The prognosis is good after complete resection of the diseased cartilage and soft tissue. Incomplete resection, however, may be complicated by recurrence of clinical signs and necessitate re-operation.1
5. Hoof Wall Resection Indications for removal of hoof wall are commonly encountered in equine practice and can be accomplished in several ways. Currently, the most common condition where hoof wall removal is indicated as part of the therapy is the structural damage and separation at the stratum medium and stratum lamellatum, commonly known as "white line disease." 1 The term "white line disease" is a misnomer because the white line is anatomically defined as the junction of the hoof wall and sole. However, "white line disease" is the most common term used to describe the separation of hoof wall proximal to the white line. White line disease seems to be a progressive deterioration of the attachment of the hoof wall that appears to be the result of keratolytic agents that have yet to be definitively identified (Fig. 6).1 This loss of attachment can occur in hooves that appear healthy on the surface and have no known injury or disease. It is not uncommon for an outwardly appearing normal hoof wall to have a significant amount of hoof wall unattached. This occurrence led to the early descriptions of "hollow hoof."1 Farriers often recognize the occurrence of unattached wall before significant damage has been done. These early cases are easily treated with removal of the diseased tissue and application of an astringent/antiseptic. If, however,the hoof wall separation is extensive, removal of the affected and undermined hoof wall is the most effective way to resolve the condition. It is common for the hoof wall to grow back completely normal and well attached. Hoof wall removal can also be useful in dealing with extensively infected and unstable hoof cracks. Removal of the diseased and undermined hoof wall can allow better resolution of the infection and facilitate treatment of the underlying sensitive tissues.1 There have been numerous methods described for removal of hoof wall with each having their application and respective advantages and disadvantages. Probably the most widely used method involves the use of a motorized tool, such as a dremel and tungsten carbide bits to remove the hoof wall or create a groove to separate diseased from normal hoof wall.1 The advantage of using a motorized burr is that it allows controlled and precise removal of tissue.The biggest disadvantage is that it can be quite slow when removal of large areas of hoof is necessary.If removal of large amounts of hoof wall is indicated, a pair of half round nippers from GE Forge can be used to do the "rough" work, and the more precise"edges" can be touched up with the motorized burr.1 Therapeutic shoeing is usually indicated to provide stability to the foot and reduce pain. After substantial hoof wall resection, instability of the distal phalanx may ensue, resulting in ventral rotation of the bone. This is best managed by application of a heart bar shoe or other appliance to attempt stabilization of the distal phalanx. After hoof wall is removed, depending on the extent of the resection,it is usually indicated to keep the hoof wall bandaged until the exposed tissue is adequately cornified and lameness has resolved. After the tissues are adequately cornified and firm to the touch, application of a composite reconstruction may be considered if needed.1 Something that has proven useful in the treatment of hooves after removing the hoof wall is the use of a sugar and betadine paste. The hypertonicity combined with the antiseptic povidone-iodine does a nice job of drying out the underlying tissues without the use of more harsh astringents. After the tissues have shrunk and dried, the bandages can be removed, and either iodine or thiamersol can be used to further harden the cornifying tissues.1 6. Subsolar Abscesses Subsolar abscesses are probably the most frequent condition affecting the foot of the horse for which invasion of the hoof capsule is required. Affected horses often present with a severe lameness, and the horse owner is often concerned that the horse has a fracture or other malady resulting in the presenting lameness.1 An increase in the strength of the digital pulse will be palpable as a result of the inflammation within the foot. Hoof tester examination may identify a focal area of sensitivity (such as over a nail hole); however, most commonly the pain identified is generalized over much of the sole. Perineural anesthesia of the palmar digital nerves just proximal to the collateral cartilages will often resolve the majority of the lameness; however, on occasion,anesthesia of these nerves at the level of the proximal sesamoid bones is necessary, particularly when the abscess is in the toe region.1 Occasionally,the pain from the abscess is not overcome by desensitizing (blocking) the foot, further confounding the diagnosis. Careful examination of the bottom of the foot will often allow identification of a tract or crack that will lead to the abscess. Often paring of the sole with a hoof knife is necessary to identify black areas that may lead to the abscess. When a crack or black area is identified, careful exploration is necessary to identify if the abscess is beneath that area. A small looped hoof knife or a #2 curette is useful to explore these areas that may potentially lead to the abscess.The crack or black area is followed by removing a small amount of hoof material until the crack or black area disappears or until the abscess is opened up. Often, a grayish-colored fluid will escape or ooze from the abscess entry site once the abscess is penetrated. The authors prefer to make just enough of an entry site that will allow the fluid to drain from the abscess cavity. A large hole is generally unnecessary; however, small holes can plug and result in recurrence of clinical signs. Large abscesses with significant undermining of the sole may need to be debrided more aggressively.1 Aftercare is routine and involves placing the foot in a bandage to keep dirt and debris from plugging the drainage hole. 7. Conclusion Surgery of the equine foot is often perceived to be quite difficult because of the hoof capsule. Knowledge of the specific disease entities that require surgical intervention and an in-depth understanding of the anatomy of the tissues beneath the hoof capsule is a prerequisite to successful surgical treatment.A close working relationship between the veterinarian and farrier needs to be established to produce optimal results. References and Footnotes
|