Farriery for the foal: A review part 2: Therapeutic farrieryReprinted with permission from Equine Veterinary Education (EVE). |
|
Conservative treatment such as restricting exercise to reduce further trauma to the foot is paramount. Correcting the nutritional status of the foal (i.e. weaning the foal to avoid possible excessive nutrition from the lactating mare and/or decreasing carbohydrate intake), administering an anti-inflammatory agent (NSAID) to relieve pain, administering oxytetracycline to foals with acquired flexural deformities to facilitate muscle relaxation and carefully trimming the palmar section of the hoof are, in the author’s opinion, is a reasonable starting point. The NSAIDs should be administered short-term and judiciously in foals due to the potential side effects, such as gastroduodenal irritation and nephrotoxicity.For analgesia, the author will administer firocoxib (0.1 mg/kgbwt q. 24 h) or flunixin meglumine (1.1 mg/kg bwt q. 24 h)combined with a gastric protectant. Hoof trimming is directed towards improving the hoof angle by lightly trimming the heels from the middle of the foot palmarly until the hoof wall at the heels and the frog are on the same plane. Over trimming of the heels should be discouraged as this will invariably cause the heels to lift off the ground which can be noted on firm footing. The bars can be thinned in this instance as an attempt to spread and possibly improve heel expansion. Additionally, the heels of the hoof capsule adjacent to the frog sulci may also be rasped to a 45° anglein an attempt to promote spreading. If the sole thickness is sufficient in the dorsal foot (does not deform with hoof testers or thumb pressure), breakover is moved palmarly by creating a mild bevel with a rasp, which begins just dorsal to the apex of the frog and extends to the perimeter of the dorsal aspect of the hoof wall (Fig 1). If improvement is noted, this trimming regimen is continued and optimally performed at 2-week intervals. If the toe is constantly being bruised or undergoing abscessation, an acrylic or urethane composite (Equilox® orVettec®) can be applied to the dorsal aspect of the sole and the distal dorsal aspect of the hoof wall to form a protective toe ‘cap’. The acrylic composite-impregnated fibreglass combination or urethane composite used to form the toecap will cover the solar surface with a thin layer of composite from the margin of the dorsal hoof wall to the apex of the frog, protecting that area from further damage and creating or exacerbating lameness. Caution is advised when a composite cap is applied as the sole-wall junction may be stretched or have separations/fissures present which make it
| ||
| ||
|
The above treatment for a mild flexural deformity is often temporary as many foals will progress to a more severe deformity and thus the farriery appears to work best when initiated at the first sign of abnormal foot conformation before a marked flexural deformity is apparent. Whenever possible, the elimination of any possible or suspected inciting causes should be pursued.The farriery for a mild flexural deformity should always be combined with restricted exercise. If the affected foot continues to improve or does not regress, conservative treatment is continued. If a mild flexural deformity progresses in severity to the stage where a marked flexural deformity is present, the foal becomes a surgical candidate.
Severe acquired flexural deformities of the DIPJ
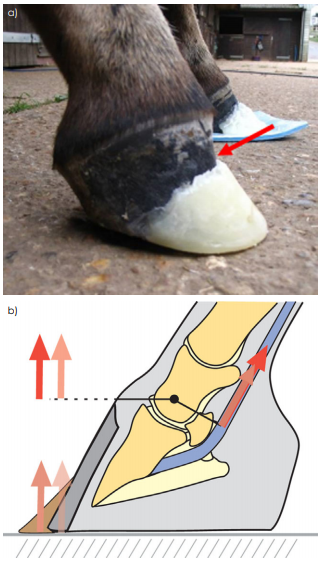
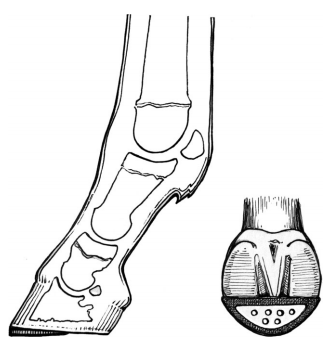
A mild acquired flexural deformity may progress in severity despite conservative treatment or a severe acquired flexural deformity may be acute in onset. A severe acquired flexural deformity is characterised by a foot with a hoof angle greater than 80°, a prominent fullness at the coronary band,a broken forward hoof-pastern axis, disparity in hoof wall growth distal to the coronet at the heel relative to growth at the toe and heels that fail to contact the ground (Fig 2). If the flexural deformity is allowed to persist, the foot eventually assumes a boxy, tubular shape due to the overgrowth of the heels to accommodate the lack of ground contact; heel length will approach the length of the toe (Fig 3). Increased stress on the hoof wall at the toe will eventually cause a concavity along the dorsal surface of the hoof wall. Stress exerted on the sole-wall junction in the toe area will cause it to widen, allowing separations to occur.
Farriers have traditionally applied toe extensions to create a lever arm using a shoe or a composite to force the heel to the ground, but this will only exacerbate damage to the dorsal section of the foot, promote hoof wall separation and delay breakover (Hunt 2012; O’Grady 2017). As it is important to consider the use of a toe extension in biomechanical terms and to understand the effect of this leverage, it is necessary to briefly consider the moments about the distal interphalangeal joint. The moments about the DIPJ are the flexor moment and the extensor moment (a moment is equal to force x distance). At rest, the extensor moment is the product of the weight born by the limb (a force) and the horizontal distance from the point at which the ground reaction force GRF acts on the foot (centre of pressure CoP)and the centre of rotation of the distal interphalangeal joint(a distance). The flexor moment opposes the extensor moment and is the product of the force (tension) in the tendon and the shortest distance of the deep digital flexor tendon (DDFT) from the centre of rotation. Normally these two moments are balanced at rest, the GRF is dorsal to the centre of rotation of the joint and the heels are on the ground. In foals with a flexural deformity of the DIPJ, the tension in the tendon increases (as a result of the shortened musculotendinous unit), which increases not only the flexor moment but the opposing extensor movement which moves the CoP dorsally in the toe. At the point where the tension in the tendon increases such that the CoP is at the dorsal limit of the toe, any further increase in tendon tension cannot be balanced by movement of the CoP because it is already at the perimeter of the toe and can't move further dorsally,therefore, the heels lift off the ground (Eliashar 2012). Adding an extension to the toe of the foot allows the centre of pressure to move further dorsally in the toe in an attempt to counteract the tension in the tendon and force the heels to the ground. The ability of the toe extension to do this is dependent on the integrity of the tissues (hoof wall,lamellae), however, the tissues are not generally strong enough to withstand the additional stress and separation occurs within the dorsal hoof wall. Therefore, placing an extension or leverage on the dorsal hoof wall to counteract the forces in the shortened deep digital flexor muscle tendon unit is unrealistic and, in the author’s opinion, contraindicated(Fig 4). Furthermore, extensions may contribute to lameness due to excessive stresses on the DDFT when the foal puts full weight on its foot and at the initiation of breakover.
|
Radiographs should be used to assess changes in the joint and the integrity of the distal phalanx. The author will administer mild sedation (xylazine [0.33 mg/kg bwt, i.v.]combined with butorphanol [0.022–0.066 mg/kg bwt i.v.]) and place each of the foal’s feet on separate wooden blocks of equal height, which allows normal or equal loading of both forefeet. The forelimbs are positioned such that the third metacarpal bone is perpendicular to the ground. Lateral-medial weight-bearing images of both forefeet should be acquired. The degree of flexion of the DIPJ, the angle of the dorsal hoof wall and abnormalities at the margin of the distal phalanx should be assessed (Fig 5). When a marked flexural deformity is noted during radiographic examination of the feet, conservative treatment and hoof trimming alone are generally unsuccessful in resolving the foot conformation.Elevating the heels has been advocated to reduce tension in the DDFT and to promote weight-bearing on the palmar section of the hoof. However, although elevating the heels will load the palmar section of the foot, improve the hoof pastern axis and make the foal more comfortable initially, the author has not been able to subsequently lower the heel or remove the wedge and establish an acceptable hoof angle with the heel on the ground. Once a marked flexural deformity of the DIPJ with the heels of the hoof capsule lifted off the ground or a distorted hoof capsule characterised by afoot with a steep hoof angle, a prominent fullness at the coronet, a broken forward hoof-pastern axis, a disparity in the length of the heel relative to the toe of the hoof and some degree of concavity in the toe is apparent; the author recommends transection of the accessory ligament of the DDFT combined with the appropriate farriery.
The farriery is generally performed prior to the surgery either before or while the foal is anaesthetised to prevent manipulating the limb and handling the surgical site following the procedure. A toe extension is not used; rather an acrylic composite is applied to the solar region of the toe to create a reverse wedge (Stone and Merritt 2009; Hunt 2012; O’Grady2012, 2017). The wedge affords protection for the toe region and appears to redistribute the load to the palmar aspect of the foot, thus mildly increasing the stresses on the DDFT, and appears to restore the concavity to the sole. The heels are lowered with a rasp from the point of the frog palmarly, until the sole adjoining the hoof wall (sole plane) at the heels becomes solid. This will generally place the hoof wall and the frog on the same horizontal plane. Any concavity or bending in the dorsal aspect of the hoof wall is removed with a rasp in order to redirect the forces directly under the coronet at breakover. The ground surface of the foot dorsal to the frog and the perimeter of the dorsal hoof wall are sanded and prepared for the composite wedge using a rasp or motorised burr (Dremel® tool). Deep separations in the sole-wall junction at the toe are explored and filled with clay, if necessary, to prevent tracts for infection beneath the composite. Foals undergoing this procedure are usually between 3 and 5 months old; therefore, due to their size and weight,reinforcing the composite with fibreglass is necessary to prevent excessive wear.
|
The surgical aftercare is at the discretion of the attending clinician. Oxytetracycline may be used with the surgery during the perioperative period to facilitate relaxation of other soft tissue structures secondarily involved (joint capsule,collateral ligaments) (Hunt 2012). Controlled exercise in the form of daily walking or turn out in a small paddock with firm footing such as a round pen is essential. There is the potential for pain with the initiation of exercise due to the shortening of soft tissue structures such as the joint capsule and suspensory ligaments to the navicular bone, requiring close monitoring of the foal, and exercise should be increased sequentially. The foal is trimmed at roughly 2-week intervals, based on the amount of hoof growth at the heels with the objective of establishing normal hoof capsule conformation. The composite wedge is removed one-month post-surgery. At subsequent trimmings, the heels are trimmed as necessary from the middle of the foot palmarly such that the frog and hoof wall are on the same plane and hoof wall at the toe is trimmed from the dorsal aspect of the hoof wall until the desired conformation is attained. No sole dorsal to the frog is removed. This type of trim promotes sole growth and creates approximate proportions on either side of the COR. When the desired foot conformation is reached, the foot is trimmed in a routine manner monthly. It is important to emphasise that when the hoof capsule returns to an acceptable conformation, only that portion of the sole that is shedding should be removed. This avoids causing discomfort in the dorsal solar section of the foot that can result in the foal redeveloping, to some degree, the original flexural deformity.The higher-grade clubfoot appears to have a tendency to revert back to the original deformity if not managed properly.
Angular limb deformities
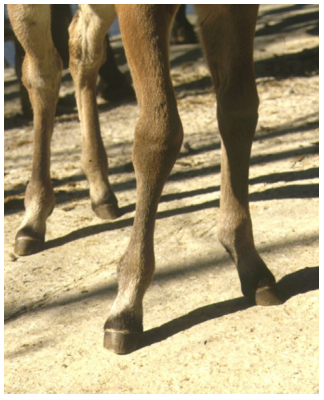
Angular limb deformities (ALD) are common in foals and require early recognition and treatment (Greet 2000; Hunt 2000; Greet and Curtis 2003; Auer 2006; Witte and Hunt 2009;Garcia-Lopez 2017; O’Grady 2017). This subject receives tremendous attention in any discussion of foal conformation and it refers to a lateral or medial deviation in axial alignment of the limbs when the animal is viewed from the frontal plane. It is understood that a certain amount of deviation can be normal in young foals and does not require any special farriery or surgical intervention (Hunt 1998, 2000; Auer 2012; O’Grady 2017). Objective data is lacking regarding the dynamics involved in the development of acquired angular limb deformities, however, it is recognised that many foals change axial alignment during various stages of their development. Serial evaluation and treatment of limb deviations is an integral component of management on most breeding operations.
Angular limb deformities may occur anytime during the animal’s life but are most commonly treated from birth through the yearling growth period. The primary lesion appears to be an imbalance of physeal growth; for assorted reasons, growth proceeds faster on one side of the physis vs.the other. Although this is described as a discrepancy of limb length of the medial vs.
|
Limb alignment of young foals should be observed standing and walking without restriction on the head and neck (not leaning) toward and away from the examiner.Overall body development and maturity should be noted. It is important to take note of foot placement especially when working with distal limb deviations. This will determine the necessity for corrective measures on the feet such as trimming or placement of a composite extension on the hoof capsule to alter the forces on the physis and change the rotation of the limb on contact with the ground. This practice is especially beneficial with a fetlock varus deviation with inward rotational deformities in foals 2–4 weeks of age in which there is a limited time frame for correction.
Carpal/tarsal valgus
It is apparent that a mild carpal valgus of 2–5 degrees offers the newborn foal a comfortable stance while nursing and eating off the ground and is considered acceptable. If the deviation exceeds 5–8 degrees then it becomes a concern and should be monitored (Hunt 1998, 2000; Auer 2012). A few days of stall confinement on firm bedding or limited exercise in a small paddock (2–3 times a day) is a rewarding, cost effective treatment for early carpal or tarsal valgus (Garcia Lopez and Parente 2011).
|
It may be helpful to digress and briefly mention routine hoof care before discussing treatment of angular limb deformities. The technique for using farrier tools when trimming foals was discussed under the trim in Part 1 of this review. The veterinary and farriery literature abounds with various trimming methods that are thought to affect the various limb conformations; however, none of these methods have been substantiated or documented to be efficacious.The author trims the heels such that the heels of the hoof wall and the frog are on the same plane, visualises a line across the middle of the foot (located just dorsal to the COR) and then reduces the toe to make the foot proportional on either side of the line across the widest part of the foot. When the trim is complete, the solar surface of the foot will be level rather than having the lateral to medial orientation of the foot changed by rasping one side of the foot more than the other (Fig 8). Farriery texts describe trimming a foal lower on the outside of the foot when the foot turns out and trimming the foal on the inside of the foot when the foot turns in;however, remembering that a toe-out or toe-in stance originates from the limb, this practice will do nothing more than place excessive stress on one side of the hoof capsule
If the angular limb deformity is greater than 5–8 degrees or shows no improvement in the first few days of life, radiographs should be part of the physical examination of a foal with ALD(Garcia-Lopez and Parente 2011; Garcia-Lopez 2017).
Occasionally, osseous abnormalities such as hypoplastic carpal/tarsal bones will preclude correction of the problem without splints or a cast. Radiographs will also reveal the site and degree of deviation which will allow comparison later.Carpal valgus deformities of less than 10 degrees are generally handled successively with conservative treatment(Garcia-Lopez and Parente 2011; Garcia-Lopez 2017).
Conservative therapy for the management of many mild to moderate congenital angular limb deformities may be successful in the newborn foal. Restricted exercise would be either strict stall confinement or brief periods of turnout (1 h two times daily) in a small area with firm footing. This allows the physis to be stimulated but prevents stress, fatigue and compression on the overloaded side of the growth plate from excessive exercise. If the carpus can be corrected by applying pressure with one hand on the inside of the carpus and counter pressure with the other hand applied to the outside of the fetlock, some form of coaptation such as support tape, splints, dynamic splints or tube casts may be helpful. The author uses a splint made from polyvinyl chloride(PVC) pipe, cut in half and fitted from the elbow to below the fetlock applied for a few hours 1–2 times daily. It is labour intensive, but the splints must be removed and replaced periodically to prevent laxity. A full-length thick cotton bandage is applied to the entire limb, and then the PVC pipe is placed on the outside of the limb and secured to the bandage with elastic tape. This will distract the carpus laterally and load the limb more proportionally. The splint is often the most cost-effective treatment available but must be applied with caution, paying strict attention to the details of application. Meticulous attention to applying the splint is essential to prevent focal pressure and the propensity of the foal to develop decubital ulcers. As the foal improves, brief periods of turnout in a small area with firm footing can be considered.
|
Acquired carpal/tarsal valgus deformities can be graded from one to four according to severity (Fig 9). Mild to moderate carpal valgus will generally respond to restricted exercise and the use of a composite extension applied to the medial side of the foot while the more severe cases require surgical intervention combined with farriery (Hunt 1998, 2000;Greet 2000; Auer 2006; Witte and Hunt 2009; Garcia-Lopez2017; O’Grady 2017). Various clinicians have described trimming the lateral side of the foot aggressively when there is a valgus deformity in an attempt to increase the ground surface on this side of the foot (Greet and Curtis 2003).However, it is this authors’ opinion that the foal does not grow sufficient horn at this age to make an appreciable difference and changing the medial to lateral orientation of the foot may have detrimental effects on the immature hoof capsule as well as the physis. Using some form of extension to increase the ground surface of the foot and change the forces on the physis seems to be more beneficial (Cheramie and O’Grady 2003; Greet and Curtis 2003; O’Grady 2017).
Periosteal elevation is a controversial surgery that is routinely performed on foals with mild to moderate angular limb deformities (Garcia-Lopez 2017). However, the author has not referred a foal for this surgery in 20 years as the author saw no difference when compared with foals that had controlled exercise (brief turnout in a small paddock with firm footing) and the application of a hoof extension(O’Grady unpublished data, 2014). If stall confinement is used initially, the mare and foal should be bedded on firm footing(such as a thin layer of sawdust) for the foot extensions to be effective. Initially, the author prefers using some form of extension to increase the ground surface area of the foot on a given side and change the forces on the affected joint.Some type of composite applied to the hoof wall is preferred rather than a cuffed shoe that is attached with glue as this type of shoe appears to restrict movement of the hoof capsule and contracts the foot especially the heels. As noted previously in Foot care in foals: A review part 1, the author will not apply a composite to a foal’s foot before 3 weeks of age because of the potential detrimental effects of the excessive heat
For carpal valgus, the composite extension is placed on the medial side of the hoof and toward the heels which appears to redirect the forces on the physis on the overloaded side of the limb by moving the axis of weight bearing towards the centre of the limb (Fig 10).
|
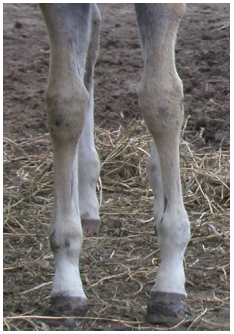
Fetlock varus
Varus deformities involving the fetlock are common in either the front or hind limb of newborn foals (Fig 11).
| ||
|
Carpal varus deviations are also recognised in young foals and weanlings. Foals that develop carpal varus from birth to 1–2 months of age often have an ‘over at the knee’ appearance and buckle forward when standing. These foals typically worsen with exercise and improve with rest. Dietary control is important as is the judicious use of analgesics and controlled exercise. Lateral extensions placed on the foot maybe useful but surgical intervention may be necessary if the varus deformity is severe. Weanlings that develop carpal varus are typically offset at the carpus, sometimes pigeon toed and often have accompanying physeal dysplasia. If the physeal dysplasia is kept under control; the deviation will often resolve.If the condition fails to respond, surgery such as transphyseal bridging or placement of a transphyseal screw in the physis of the distal lateral radius may be necessary. In general, valgus deviations are far easier to manage and are more prone to spontaneously correct and appear much more forgiving from a soundness standpoint than varus deviations.
Conclusions
The concept of protecting the foot from the deleterious effects of mal-loading created by many FLDs and ALDs is just as important as using the symptomatology as an instrument to correct the deformity. Flexural and angular limb deformities are often controversial and have a multitude of purported treatments; it is therefore essential that appropriate communication occur among the responsible parties to avoid any misunderstanding and unnecessary or job threatening miscommunications. Management of limb deformities in foals, irrespective of the type, severity or origin,are best managed through a coordinated effort between the owner, farm manager, farrier and veterinarian. When treating valgus and varus limb deformities especially fetlock varus, prompt early recognition and treatment is best for consistent correction. Most veterinarians are not able to perform the farriery required to address foot and limb issues in foals, so their reliance on a farrier becomes obvious. A veterinarian not well versed in farriery should familiarise themselves with good basic farriery and have a working knowledge of this discipline. An avenue of communication between the professions is not only necessary but mandatory.Hoof care in the first few months of life is serious business and should never be taken lightly. Appropriate farriery combined with medical/surgical input from the veterinarian is essential when confronted with orthopaedic disorders related to the limbs. Farriery plays a vital role in both the development of the hoof and the conformation of the limb. A planned foot care programme is time consuming whereas assembly-line trimming is quick and easy, but the former thoughtful approach is much more rewarding with a better outcome
Conflict of Interest
No conflicts of interest have been declared.
Not applicable.
Declaration of EthicsNot applicable.
Source of fundingNone.
REFERENCES