An In-Depth Look at Puncture Wounds to the FootReprinted with permission from the American Association of Equine Practitioners. Originally printed in the 2010 AAEP Convention proceedingsW. Rich Redding, DVM, MS, Diplomate ACVS 1. Introduction The horny hoof capsule of the foot is typically resistant to wounding, but under the right circumstances,sharp objects can penetrate the sole and frog. The skin above the coronary band, however,is commonly involved in entrapment wounds, lacerations,and puncture wounds of the distal limb.Wounds to the solar surface of the foot most often occur when the horse steps on a sharp object(s), such as a nail. Puncture wounds have been classified according to the depth of penetration (superficial and deep) and location on the foot.1-3 Superficial wounds penetrate only the cornified tissue, whereas deep wounds penetrate the germinal epithelium. However, wounds to the sole need only to penetrate1 cm to invade germinal epithelium, whereas wounds of the frog may need only 1.5 cm to invade vital structures. Fortunately, the most common wound is a superficial wound of the solar surface of the foot. Deep wounds are much more serious and separated into three types based on location. Type I wounds penetrate to the sole and may damage the distal phalanx (P3), whereas Type II wounds penetrate the frog and heel and can involve the deep digital flexor tendon (DDFT), distal sesamoidean imparligament (DSIL), navicular bursa (NB), distalinterphalangeal joint (DIPJ), digital flexor tendon sheath (DFTS), and digital cushion (DC). Type III injuries penetrate the coronary band and may cause septic osteitis of P3, septic chondritis of the collateral cartilages of P3, or septic arthritis of the DIPJ. Because deep wounds have an increased risk for serious consequences, the need for early identification of structural involvement and the institution of aggressive medical treatment and early surgical intervention cannot be overemphasized. Assuming that the wound is superficial may promote a delay in the institution of the most appropriate treatment and may be the difference between humane destruction and return to soundness. This paper will discuss the varied clinical presentation, diagnostic work-up, and treatment options of puncture wounds to the foot. 2. Clinical Presentation and Diagnosis Puncture wounds, whether superficial or deep, can frequently create marked lameness. The degree of lameness may vary considerably depending on the depth, location, and duration of the wound. Superficial wounds may have minimal lameness initially but become more severe several days later with the development of abscessation. In general, puncture wounds that invade the corium become quite painful soon after wounding. Progression to severe non weight-bearing lameness occurs as the rigid horny hoof capsule restricts the swelling associated within flammatory response. Wounds that involve deeper structures such as P3 or any of the synovial structures such as the NB, DIP, DFTS, and/or the DDFT often become rapidly symptomatic. Unfortunately, the depth that these objects penetrate past the horny hoof capsule can be difficult to ascertain,and the severity of the clinical signs do little to help define the structures that are involved. Recognizing when the wound occurred and where the wound is located can assist the clinician to choose the most appropriate diagnostic and treatment strategy. A detailed history combined with a careful clinical examination is critical to direct the use of diagnostic imaging (radiography and ultrasonography) and assess the need for clinical pathological analysis of joint/bursa/sheath fluid (should the potential for synovial sepsis exists). Magnetic resonance (MR)may be necessary to more accurately determine the extent of the injury.4
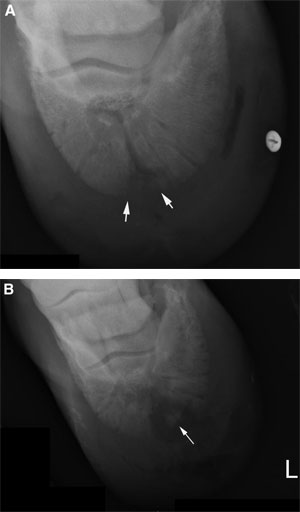
Many horses point the affected limb and preferentially load the unaffected area(s) of the foot when walking. Increased digital pulses are common, and in some cases, the digital pulse may be increased only on the affected side. Increased heat may be palpable at the coronary band and/or over the hoof capsule in the affected limb. With chronicity, there may be swelling of the pastern, and a non-septicef fusion within the digital flexor sheath can develop because of a sympathetic flare associated with the inflammatory response within the foot. Hoof-tester application, early after wounding, may reveal pinpoint sensitivity, but over time, a painful reaction may be elicited over the entire sole region. Visual inspection of the foot will often reveal the source of the lameness and should begin by cleaning of the hoof wall, sole, and frog. If the offending object remains in the foot (especially radio-opaque material),an attempt to obtain a set of radiographs can allow the clinician to measure the depth of penetration and evaluate which structures may be involved (Fig. 1). Paring the sole with a hoof knife or rasping the hoof wall may reveal the puncture wound or a black tract or crack in the solar surface. After the surface of the foot is cleaned and the wound is identified, a sterile preparation of the foot with an antiseptic detergent and alcohol rinse should be performed. This will allow further exploration of the wound without fear of contaminating the surrounding normal tissue. Probing of the wound with a sterile probe or teat canula can be helpful to determine the depth and direction of the wound. Radiographs taken with the probe/canula in place can more accurately assess depth and direction and the structures affected. When an obvious crack or black tract is found, then exploration may lead to an abscess. A small looped hoof knife or a bone curette (#2) is useful to explore these areas and establish drainage. Locating the entry site of wounds to the frog may prove difficult, because the elastic tissues of the frog tend to close over the wound. After cleaning the foot, if a wound is not apparent, then hoof testers should be applied in a methodical manner to find point sensitivity suggestive of the puncture site. Sharp debridement of the wound is necessary to remove necrotic tissue as well as any foreign material that is present in the wound. The depth of the sharp dissection is determined by the appearance of the tract and is guided by placement of a sterile probe. Radiography is indicated in all cases to identify the presence of concurrent bony involvement such as fractures, osteitis, and later sequestrum formation.Gas shadows, debris, and radio-opaque foreign bodies may be seen, and this may indicate the depth and direction of the puncture. More advanced radiographic diagnostic techniques such as contrast fistulography or contrast arthrography may be necessary to evaluate a poorly defined wound and to more carefully assess the specific structures (especially synovial) that may be involved. The technique and indications for these procedures will be discussed later in the paper. Osteitis and sequestrum formation may take weeks to manifest radiographically,and therefore, follow-up radiographs may be indicated if the wound is not healing appropriately.Diagnostic ultrasonography has also proven particularly helpful to define the extent of damage incurred during wounding, either from a puncture or laceration of the distal limb. Use of diagnostic ultrasound can be helpful to assess wounds to the foot but is limited to windows provided by the skin at the coronary and softer tissue of the frog. Given this limitation, diagnostic ultrasound has been helpful to identify tendon damage and synovial distention as well as assess the character of the synovial fluid of the DIPJ, NB, and DFTS. An increase in cellularity and fibrin content in the synovial fluid increases its echogenicity.The presence of gas shadows suggests either an open joint space or the presence of gas-producing organisms in the joint fluid. In addition, shadowing artifacts may be visible ultrasonographically, which is suggestive of foreign material such as wood splinters commonly seen in coronary-band wounds. The specific use of diagnostic ultrasound will be discussed where appropriate later in the paper. Clinical pathological evaluation of the synovial fluid of the NB, DIPJ, and/or DFTS is often necessary to confirm synovial sepsis. With the needle in position in the joint, it can be beneficial to inject sterile balanced electrolyte solution in a volume significant to generate substantial fluid pressure within the joint. A positive fluid-pressure study evidenced by visualizing fluid escaping from the wound is strongly suggestive that the integrity of the synovial capsule has been compromised. The synovial structure(s) should be considered contaminated and potentially septic. Early diagnosis and aggressive treatment are critical to effectively treat wounds that invade the NB, DIPJ, DFTS, and DDFT, and therefore, it warrants these diagnostic procedures. Wounds to the coronary band are managed similarly with joint-fluid recovery and a fluid pressure study performed on the DIPJ (if the wound is dorsal) and DFTS (if the wound is palmar/plantar),and they should be carefully assessed for a foreign body, particularly wood splinters. Reconstruction of these wounds should be attempted where possible. Penetrating objects are commonly contaminated with dirt, rust, and manure. This material is driven deep into the wound. The superficial aspect of the wound frequently seals quickly. Without adequate drainage, an anaerobic environment develops and can promote the growth of anaerobic bacteria. Abscessation formation is common and will require drainage. Although this abscessation can easily be drained, one organism of particular concern that can be deposited in the tissue is Clostridiumtetani, which causes tetanus. This disease is not often treated successfully, and therefore, it is better prevented by vaccination. Adequate protection can be achieved by vaccination with tetanus toxoid; however, a booster of toxoid should be given in the event of a puncture wound to the foot. Unvaccinated horses should receive both a tetanus toxoid and a tetanus antitoxin as soon after wounding as possible. Farriers may be asked to deal with puncture wounds to the foot. Superficial wounds carry a good prognosis and can have dramatic resolution of lameness within 24-48 h, whereas deeper wounds require surgical debridement. Superficial wounds and infections are effectively treated by establishing drainage, soaking the foot in an Epsom-salt solution,poulticing the foot until drainage has ceased, and protecting the foot until the hoof-capsule defect has healed. Because of the serious complications that can occur with the deeper wounds mentioned earlier in this paper, it is this author's opinion that a veterinarian should be involved when dermal tissue has been affected and debridement of this tissue is necessary. Any delay in the initiation of the appropriate treatment can have serious consequences.Debridement may be painful and necessitates the use of diagnostic analgesia at the level of the palmar digital or abaxial sesamoid nerves. In addition, the procedure may cause hemorrhage, which can be minimized when a tourniquet is applied. Regional perfusions are becoming more frequently used to increase the concentration of antibiotics in the foot,and they require a veterinarian to perform. Medications such as antibiotics and anti-inflammatory drugs may be indicated and will need a veterinarian's prescription. If a farrier were to treat an established infection in the hoof, it could be perceived as practicing veterinary medicine, and the farrier could be held liable
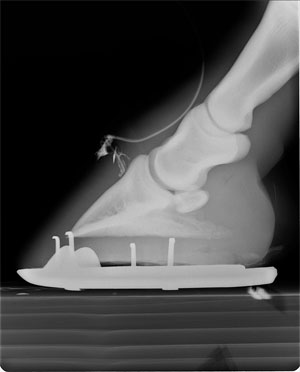
3. Septic Pedal Osteitis and Sequestrum Puncture wounds to the sole of the foot can introduce bacteria and debris to the solar surface of theP3 and frequently produce a septic pedal osteitis.Septic pedal osteitis involves bone lysis of P3 andoften has the presence of purulent exudate (which differentiates this condition from non-septic pedalosteitis).5 In addition, chronic soft-tissue infection(e.g., subsolar abscess from a previous puncture) can also extend into the bone. Septic pedal osteitis can also occur as a sequela of chronic laminitis. The concurrent presence of periosteal trauma, bacterial contaminations, and poor vascularity of fracture fragments result in an increased incidence of sequestrum formation and osteitis in P3. Clinical examination is similar to other puncture wounds and frequently reveals a draining tract that leads to P3. Occasionally, a horse that is on systemic antibiotics and anti-inflammatories will not manifest significant lameness and drainage until the medications/antibiotics are discontinued. However, radiographs should show the affected area to determine the presence of an osteitis and/or sequestrum (Fig. 2). If necessary, a fistulogram can be performed to evaluate the tract for a foreign body and/or to assess the amount of undermined sole. A venogram may be performed to assess blood flow to the affected area. Surgical drainage and debridement of the infected bone and necrotic soft tissue is necessary for the wound to heal. Wounds to the sole can be safely explored and debrided with the horse standing.The horse should be placed on systemic antibiotics and anti-inflammatories before surgery. An area of sole 1-2 cm in diameter should be removed around the puncture site so that the tract can be completely explored, unless radiographs suggest that the osteitis/sequestrum is determined to be larger. The surgical approach should follow the draining tract (if present) and allow adequate exposure of all affected tissue for the removal and effective ventral drainage of exudate. Complete resection of the draining tract is important. If there is no draining tract,then a radiograph with radio-opaque markers can be placed on the sole, and a radiograph can be taken to map out the approach to the affected bone. A tourniquet placed at the fetlock and proximal sesamoid bones should be used to minimize bleeding and allow the surgeon to distinguish between normal and abnormal tissue. A regional perfusion with antibiotics can also be performed after tourniquet placement and before beginning surgery. Wounds that penetrate the solar corium should have the affected corium removed by sharp dissection. Abnormal bone should be removed by curettage. Culture of the infected bone should determine the appropriate antibiotic therapy, although a mixed growth of several bacterial species can be expected. Removal of all infected/affected material is important for resolution of the drainage. After surgery, a sterile bandage is maintained during recovery and changed daily to effectively remove excess drainage. Daily inspection of the surgery site is helpful to determine if further debridement is necessary. After 5-7 days, a treatment plate may be placed on the foot to assist in daily bandage changes. Maggot debridement is anon-traumatic, minimally invasive method to remove necrotic tissue from an extensive foot infection.This therapy is often used in conjunction with and after light surgical debridement. Maggot therapy decreases healing time in postsurgical coffin bone debridements and is useful in treating chronic, reoccurring non-healing foot ulcers, canker, quittor (necrosis of collateral cartilage), chronic soft-tissue abscess, and osteomyelitis.6 The prognosis for soundness depends on the cause of the infection, its duration, and the adequacy of surgical debridement. One report evaluated that up to 25% of the coffin bone can be removed and potentially become sound.7
4. Penetrating Injuries to the Navicular Area Penetrating injuries to the frog can extend to the DDFT and depending on the direction, can extend into the NB, DIPJ, and/or DFTS. These injuries are considered potentially career-ending and even life-threatening, because sepsis within any of these synovial structures carries a guarded to poor prognosis. Sepsis of any synovial structure requires immediate and aggressive treatment. Therefore, because wounds to this area have the potential to involve these synovial structures, careful evaluation for synovial involvement is warranted. If a radioopaque foreign body is still in place, survey radiographs may help determine the depth of penetration. A complete set of survey radiographs is necessary to evaluate the depth and direction of the foreign body as well as the involvement of the soft tissues and bones of the foot (see previous discussion). At least two radiographs taken in orthogonal planes with the probe in place are necessary to define the correct depth and direction of the penetration.If the object has been removed before examination,then careful scrutiny of the foot may reveal the puncture site. A sterile metal probe can be used to evaluate the course and extent of the wound (Fig. 3). Contrast fistulography and contrastarthrography/bursagraphy are radiographic techniques that can be used to further define the wounds' involvement with the DDF and the synovial structures. Contrast fistulography is useful to assess the depth and direction of the tract by placing a catheter into the wound and injecting contrast material under pressure. The path that the contrast travels typically follows the path of the puncture wound (Fig. 4). Contrast arthrography/bursagraphy is performed by injecting contrast materialinto the DIPJ, NB, or DFTS independently to show synovial-membrane integrity (Fig. 5). If the wound has breached one of these synovial structures, the contrast material may be seen to leak from the synovial space into the subcutaneous tissues and the tract. Diagnostic ultrasound can be useful in assessing wounds that involve the frog. Careful evaluation with the probe on the frog may show gas shadows present in the soft tissues of the foot, NB, or coffin joint and should be considered confirmation of penetration and probable contamination. Diagnostic ultrasound can also be used in conjunction with probe or needle placement, because a metal content from each creates a shadowing artifact that can be visualized and followed in real time to determine the involvement of key structures. In addition, sequential ultrasonographic examinations may be used to assess the response to therapy as evidenced by changes seen in the character and quantity of the synovial fluid. Placement of a closed-suction drain at the distal-most extent of the sheath may be assisted by the use of ultrasound. This is particularly important to evaluate the effectiveness of a closed suction apparatus in collecting the accumulating fluid formed within the DFTS. Aseptic collection of a joint-fluid sample at a site remote from the wound is recommended in all cases. An increase in total cell count (>30-40,000 cells/µl) with a predominance of neutrophils and an elevated total protein concentration (≥3 g/dl) are good indicators of sepsis. Gram staining of the joint fluid may show free bacteria in the joint fluid. The fluid should be submitted for bacterial culture and antibiotic sensitivity testing. Samples of synovial fluid from the coffin joint, DFTS, and NB should be obtained. Even if one or more of these structures is contaminated, the prognosis is improved by early diagnosis and immediate and aggressive medical and surgical therapy. Medical therapy includes broad-spectrum systemic antibiotics, appropriate surgical debridement (both endoscopically and of the wound), copious lavage of the synovial structure, regional perfusion of antibiotics, and intra-articular antimicrobial medication. The diagnostic findings dictate which surgical procedure is performed. With wounds involving the frog that are not thought to involve a synovial structure, the cornified tissue overlying the puncture site should be removed, and the tract should be explored to its limit. A probe or the injection of new methylene blue dye into the tract can be used to guide dissection. Wounds thought to involve any of the synovial structures of the foot should be approached endoscopically for debridement and lavage.This procedure must be performed under general anesthesia. At the same time, regional perfusion with an appropriate antibiotic can be performed. Endoscopic examination of these synovial structures has been described elsewhere.8 In addition to endoscopic debridement and lavage, the site of wounding is debrided by sharp dissection, and all devitalized tissue is resected. After completion of the procedure, an antibiotic is injected into the affected synovial structure.
In years past, infections of the NB have been managed by a procedure termed a “street nail” surgery.This procedure involves creating a funnel shaped window in the frog with a layer by layer dissection through the DC to expose the DDFT.In the process, all devitalized tissue around the puncture wound is debrided (Fig. 6). If the puncture wound seems to continue through the DDFT, then a longitudinal incision that separates the tendon fibers is made in the DDFT to allow exposure to the NB. Any portion of the tendon that appears necrotic or devitalized is resected. The NB is opened and lavaged. Careful placement of the window through the DDFT over the flexor cortex of the navicular bone is critical to avoid entering the coffin joint distal to the navicular bone (through the impar ligament) and the palmar/plantar pouch of the coffin joint or the DFTS proximal to the navicular bone.The flexor tendon sheath and coffin joint should be distended to determine if there has been inadvertent penetration of either structure. Postoperative care is a very critical aspect of this streetnail procedure. Lavage of the bursa/joint/sheath and both regional perfusion and intra-articular/intrathecal antibiotics should be performed daily for 3 days and then every other day for 3 days until clinical improvement is seen. The surgical wounds and the dissected frog wound should be maintained under a sterile bandage and changed daily until the discharge begins to diminish. Convalescence after the streetnail procedure is much longer than for horses treated using endoscopic lavage of the NB. The streetnail wound will take substantially longer to fill in and will require much more frequent and intense postoperative care. For those horses that require a streetnail procedure, a cancellous bone graft can be packed into the wound to promote the obliteration of dead space, prevent ascending contamination, and provide a scaffolding into which cells can migrate during wound healing.
When financial constraints limit more involved therapy, transcutaneous lavage of the NB, with ingress/egress of fluid and antibiotic through an 18-gauge, 3.5-in spinal needle, can be attempted (Fig. 7). However, it is important to impress on the clientthat this procedure is likely to be effective onlyin early cases with minimal contamination, andeven then, the success rate is much lower than forsurgical exploration and lavage. In an early report, horses with NB sepsis treated with appropriate surgical debridement within 4days after injury had a reasonably good prognosis.Another author has reported good success with arthroscopic exploration of the NB in lieu of the more aggressive streetnail procedure. Cases involving a hindlimb are more likely to return to previous activities than those involving a forelimb. When the DDFT is involved, the prognosis is more guarded.The most common and serious mistake made in the management of these cases is the initial use of a conservative approach. 5. Lacerations and Penetrating Injuries That Involve the DIPJ Septic processes involving the DIPJ usually result from traumatic injuries to the foot, most often a laceration that involves the dorsal aspect of the coronary band. Puncture wounds to the frog can penetrate the DDFT, NB, and DIPJ, creating a septic bursa and joint. Diagnosis and treatment of synovial sepsis was discussed in the previous section on penetrating injuries to the navicular area. The differences in diagnosis and management of a laceration that involves the DIPJ will be discussed here. An accurate history should be obtained to determine the time lapse since the injury, any knowledge of the wounding incident (for example, what caused the wound), the amount and character of drainage from the wound, and the degree of lameness that the horse has manifested since injury. Information about how the wound has been treated, particularly the use of any medications, is extremely important. Lacerations that involve the DIPJ (and any joint, for that matter) can be surprisingly comfortable if the joint is draining and currently being treated with antibiotics and non-steroidal anti-inflammatories.Recognizing the location of the wound and the increased risk for damaging the joint capsule in the dorsal aspect of the foot should lead the clinician to perform diagnostic procedures that can confirm or refute joint-capsule involvement. Radiographic examination of lacerations of the coronary band area with sepsis of the DIPJ may show evidence of joint-space widening because of fluid accumulation and occasional gas shadows in the joint space (suggesting that the joint is open or has a gas-producing organism). However, this radiographic finding can be inconsistent; particularly, if the joint is open, there is little accumulation of fluid. In addition to fractures, osteochondral fragments or radio-opaque foreign material may be apparent in the joint, but more often, they are close to the puncture/wound. Osteomyelitis may be evident in chronic cases. Contrast arthrography may help document joint involvement, although arthrocentesis, joint-fluid analysis, and a fluid-pressure study may be more useful than arthrography. Diagnostic ultrasound can be useful to identify synovial distention and assess the character of the synovial fluid. Demonstration of a large fluid pocket can be quite useful for ultrasound guidance of needle placement into the pocket, increasing the chance of joint-fluid recovery. An increase in cellularity and fibrin content in the synovial fluid increases its echogenicity. The presence of gas shadows suggests either an open joint space or the presence of gas-producing organisms in the joint fluid. The puncture site/wound itself should be evaluated ultrasonographically to get an appreciation of the soft-tissue structures involved and if foreign material is still present within the wound. Sterile preparation of the wound with the application of sterile lube into the wound will allow a more complete ultrasound examination of the wounded area. A sterile sleeve/glove placed over the transducer can allow placement of the probe directly over and/or into the wound to more carefully examine the specific structures that are involved. In addition,ultrasonographic diagnosis of periarticular involvement of tendon and ligament injury can significantly affect the prognosis. While placing a needle for sample collection, it is advisable to assess the integrity of the joint capsule by injecting sterile balanced electrolyte solution (BES) into the joint. The fluid should be injected under pressure, and the wound should be assessed for fluid leakage. Sometimes it is necessary to have the horse walk a short distance to visualize fluid being expressed from the wound. Fluid seen exiting the wound is evidence of capsular disruption. As discussed in the previous section, confirmation of joint contamination indicates the need for aggressive medical and surgical therapy. Arthroscopy has been reported for the treatment of septic joints and has proven to be a very useful adjunct in the treatment of joint sepsis by allowing volume flushing of the joint and extensive debridement of the affected synovial membrane. Arthroscopy allows a more complete evaluation of the joint and extensive debridement of the affected synovial tissue, especially with motorized instrumentation. Osteochondral fragments and areas of osteomyelitis are more effectively managed with arthroscopic techniques. Arthroscopic techniques are described in detail in a number of surgical texts. Arthrotomy incisions have been used in the past to treat contaminated joints but have proven inferior to arthroscopy because of the limited visualization and ability to debride the joint. However, enlargement of the arthroscopy portals to make arthrotomy incisions maybe indicated in grossly contaminated wounds to allow constant drainage of septic fluid but also to provide easy placement of a teat canula or catheter for volume flushing in the standing animal. In joints with large-volume redundant joint capsule(necessary for a wide range of motion) like the DIPJ, placement of antibiotic impregnated polymethylmethacrylate (AI-PMMA) beads or cylinders may be used to increase the local delivery of antibiotics. A recent report evaluated the use of endoscopic lavage in the treatment of septic joints, tendon sheaths, and bursae. Endoscopic portals and traumatic wounds were closed primarily after lavage. Follow-up information on the 118 patients revealed a 90% survival rate, with return to athletic function in 81% of horses.9 In this population of cases, it was the early institution of treatment that allowed this protocol to be successful. This approach is unlikely to be successful in horses with more chronic wounds that contain large amounts of fibrin and gross contamination. Long-term survival in chronic cases of septic arthritis is considered poor (only around 40% in one study).10,11 Ankylosis can occasionally and may ultimately result in pasture soundness. Use of cancellous bone grafts can help encourage ankylosis if that is the goal. 6. Infection of the Collateral Cartilages Lacerations, punctures wounds, abscesses, and occasionally,hoof-wall cracks can involve the collateral cartilages of the foot. Wounds that involve the collateral cartilage may cause cartilage necrosis, which may lead to chronic infection of the cartilage. Infection of the collateral cartilage(s) of the foot is called quittor and is most common in draft breeds. A chronic non-healing wound or abscessation with intermittent purulent discharge from the infected cartilage is the usual clinical presentation. The diagnosis is based on the clinical signs of swelling and drainage from the affected cartilage. The primary differential diagnosis is chronic foot abscess. However, the drainage site for quittor usually is above the coronary band, whereas most submural abscesses (gravel) drain from the coronary band. Lameness can be severe, especially when pressure increases from the accumulation of purulent material in the infected structures. As with foot abscesses, after drainage occurs, the lameness seems to diminish. The collateral cartilages have a poor blood supply, and therefore, healing of these tissues is slow. Furthermore, because most of the cartilage lies within the hoof capsule, it is difficult to establish effective drainage. Thus, quittor is a surgical disease.The treatment of choice is surgical excision of all infected tissue and establishment of adequate ventral drainage in conjunction with broad-spectrum antimicrobials. The wound should be cultured, but it is likely to grow a mixed population of bacteria. The surgeon can culture the infected cartilage when removed at surgery, which will give a more accurate culture and sensitivity. A proximally based curved incision is made to access the infected cartilage. Meticulous dissection is necessary, because the palmar pouch of the DIPJ is located just axial to the collateral cartilages.Honnas et al.12 recommend placing the foot in traction to place tension on the joint capsule, thereby retracting it away from the area of dissection.12 Surgical dissection can also be assisted by injecting new methylene blue into the draining tract to clearly identify the affected tissue. Complete removal of all diseased cartilage may necessitate removal of a portion of the proximal hoof wall, which can be performed with a Dremel tool or trephine, while taking care to preserve the germinal tissue of the coronary band. After the dissection is complete, the DIPJ should be distended with sterile BES, and the wound should be assessed for fluid leakage that would indicate loss of integrity in the joint capsule. If the DIPJ capsule is breeched, then the prognosis is decreased,and the joint should be treated as if contaminated.If the joint capsule can be closed, then an attempt should be made to do so. If closure is not possible, the wound should be treated as an open arthrotomy, as described for septic arthritis. The skin incision is closed primarily, if possible. The prognosis is guarded, because it can be difficult to remove all of the infected tissue. The incision is at risk of dehiscence, which can complicate those cases where the coffin joint was invaded while attempting to remove the affected tissue. If the coffin joint is invaded, then treatment becomes much more aggressive and must address the principles previously discussed. 7. IV Regional Perfusion for Septic Processes in the Digit Infection can be a serious complication in wounds involving the foot. Foot infections can be difficult to treat, because they often are polymicrobial; additionally, the organisms may be resistant to multiple commonly used antibiotics, and the infected area may be poorly vascularized (owing to its inherent structure and/or because swelling of the infected soft tissues within the rigid hoof capsule impedes vascular flow). Infection is enhanced in the presence of damaged tissue, hematoma formation, avascular bone, or foreign material (including soil and fecal matter). Sepsis, vascular compromise, and a drop in pH as a consequence of inflammation and ischemia may prevent adequate delivery or activity of antibiotics in the infected tissue. Furthermore, vascular compromise increases the risk of sequestrum formation, which can promote bacterial proliferation. IV regional perfusion (IVRP) involves the delivery of an antibiotic to a selected region of the limb through the venous system. The infused volume is delivered under pressure to ensure distribution of the fluid to all vascular spaces in the region distal to the tourniquet. Retention of the antibiotic in the venous space for several minutes allows diffusion into surrounding tissues that may otherwise have inadequate blood flow. During IVRP of the distal limb, it is possible to achieve antibiotic concentrations in the tissues that are 25-50 times the minimum inhibitory concentration required to kill most pathogenic bacteria.13 Thus, with this technique,it is possible to achieve therapeutic concentrations of antibiotic, even in necrotic tissue.
8. Technique Regional perfusion of the digit can be performed in the standing horse.14 The skin over the medial or lateral digital vein is aseptically prepared. A catheter is aseptically placed in the digital vein;most clinicians use a 20-gauge catheter placed in the lateral digital vein. A tourniquet or Esmarch's bandage is applied to the fetlock (Fig. 8). An extension set is attached to the catheter, and infusion is begun. Ideally, the antibiotic chosen is determined by culture and sensitivity results. Frequently, however, the results are not available when the first perfusion is performed. The clinician must, therefore, rely on clinical judgment and select an appropriate antibiotic based on the most likely organism(s) involved. The antibiotics most commonly used for IVRP include amikacin (0.5-1.0 g), gentamicin (1 g), potassium penicillin (10 millionunits), timentin (1 g), and cephazolin (1-2 g). Regardless of the antibiotic selected, the amount to be delivered (e.g., 1 g amikacin) is diluted in 20 ml of sterile BES. The antibiotic solution is infused over30-60 s, but the tourniquet is left in place for a total of 20-30 min before it is removed. IVRP can be performed as a single treatment or repeated as often as necessary until clinical improvement is seen or the patency of the digital veins becomes compromised. The most common complication with IVRP is injury to the vasculature and soft tissues,either from catheterization or perivascular leakage of the solution and subsequent local reaction. 9. Intraosseous Infusion Intraosseous regional perfusion is an alternative to IVRP. It has the advantage of avoiding the repeated use of regional vessels. With this technique,the antibiotic solution is infused into the intraosseous space. After aseptic skin preparation, local anesthesia,and a stab incision through the skin and periosteum, a 4-mm diameter hole is drilled through the cortex of the bone adjacent to the septic process.An intraosseous infusion needle or the male adaptor of an IV extension set is wedged into the hole, and the antibiotic solution is infused into the medullary cavity. Unfortunately, the bones of the digit can be difficult to access for this procedure. References
|