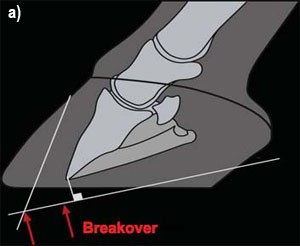
The wooden shoe as an option for treating chronic laminitisReprinted with permission from Equine Veterinary Education (EVE). Original published in Equine Veterinary Education Vol 21 Febuary 2009.S. E. O'Grady* and M. L. Steward† Summary Various farriery methods have been described for treatingchronic laminitis, yet no particular method has becomethe preferred choice. The wooden shoe may possesscertain advantages such as redistributing load evenly overthe palmar/plantar section of the foot due to its flat solidconstruction and the mechanics (bevelled perimeter,breakover and heel elevation) that can be incorporateddirectly into the fabrication of the shoe. It should beapparent that the advantages of this farriery option willalso be limited unless strict attention is paid to the detailsinvolving radiology, foot preparation and alignment of thedistal phalanx within the hoof capsule. Introduction Chronic laminitis is a frustrating and often dishearteningdisease for veterinarians, farriers and horse owners tomanage. Our ability to rehabilitate horses with laminitis,despite the type of farriery employed, is related to theseverity of damage to the lamellae (Hunt 1998). For thisreason, treatment failures with any given methodology arecommonplace. Chronic laminitis is defined by thepresence of mechanical collapse of the lamellae anddisplacement of the distal phalanx within the hoof capsule(Hood 1999). The various forms of displacement of thedistal phalanx recognised are: dorsal capsular rotation,distal displacement (sinking) medial or lateraldisplacement of the distal phalanx or any combination ofthe above (O'Grady et al. 2007a; Parks and O'Grady2008). The most common type of displacementencountered is dorsal capsular rotation. If dorsal capsularrotation is severe, the instability of the distal phalanxcombined with the weight of the horse often leads toprolapse of the sole or penetration of the distal phalanxthrough the sole. The wooden shoe has become anotherfarriery option that has been found to be a consistentlysuccessful method to address dorsal capsular rotation(Fig 1) (Steward 2003; O'Grady et al. 2007a). The woodenshoe allows the distal phalanx to be realigned, has all themechanical components of other farriery systemspreviously advocated for the treatment of chronic laminitisyet may possess many additional advantages overprevious methods used. One major advantage may be itsability to distribute weightbearing evenly over a specifiedsection of the foot due to its flat solid construction. Other advantages are:
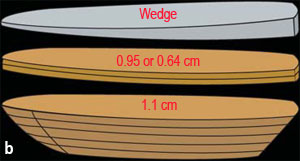
Radiology The lateral radiograph has always been considered the 'gold' standard for evaluating chronic laminitis but it does not allow identification of asymmetrical medial or lateral distal displacement (O'Grady et al. 2007a; Parks and O'Grady 2008). Therefore, the authors consider it crucial that a dorsopalmar (0° dorso palmar) radiographic projection must be included as part of the radiographic study for either acute or chronic laminitis. This allows the examiner to evaluate the distal phalanx in both a dorsalpalmar plane and a medial-lateral plane. High quality radiographs are required to visualise the osseous structures within the hoof capsule as well as the hoof capsule itself. Radiopaque markers can be used to determine the position of the distal phalanx in relation to surface landmarks. The radiographic features of chronic laminitis are well documented (Redden 2003). The following observations from the lateral radiograph are important in assessing the severity, determining the prognosis and guiding treatment: the thickness of the dorsal hoof wall; the degree of dorsal capsular rotation; the angle of the solar surface of the distal phalanx relative to the ground; the distance between the dorsal limit of the solar margin of the distal phalanx and the ground; and the thickness of the sole. The dorsopalmar radiograph is examined to determinethe position of the distal phalanx in the frontal plane.Asymmetrical distal displacement of the distal phalanx oneither the lateral or medial side is present if an imaginaryline drawn across the articular surface of the distalinterphalangeal joint or between the solar foramina of thedistal phalanx is not parallel to the ground, the joint space is widened on the affected side and narrowed orcompressed on the opposite side, and the width of thehoof wall appears thicker than normal on the affectedside. If the position of the coronary band is visible on theradiograph, then the distance between the coronaryband and the palmar processes of the distal phalanx willbe greater on the affected than the unaffected side (Fig 2). The aetiology, diagnosis and management ofasymmetrical distal displacement of the distal phalanx willbe considered in a subsequent paper. Goals of treatment for chronic laminitis Trimming and shoeing has always been the 'mainstay' of treating chronic laminitis and is directed towards reducing/removing the adverse forces on the compromised lamellae. In considering hoof care in horses with chronic laminitis, there are 3 goals for therapy: to stabilise the distal phalanx within the hoof capsule; tocontrol pain; and to encourage new hoof growth toassume the most normal relationship with the distalphalanx as possible. Realignment of the distal phalanx tocreate a better relationship of the solar surface of thedistal phalanx with the ground is used as the basis fortreating chronic laminitis (Redden 1997; Parks 2003;O'Grady 2006). Applying the wooden shoe following thisprocedure compliments the realignment of the distalphalanx and appears to decrease the forces on thelamellae due to the bevelled perimeter of the shoe. Thesame shoeing principles are applied to the wooden shoes that are applied to other shoeing methods used in treatingchronic laminitis which are to recruit ground surface,reposition the breakover palmarly and to provide heelelevation as needed (Parks 2003; O'Grady 2006). Construction of the shoe The authors chose wood due to its accessibility, lightweight, the ease with which it can be constructed andshaped (both before and after application) and its abilityto dissipate energy at impact while remaining rigid (Reid1994; Steward 2003; O'Grady et al. 2007a). The woodenshoe can be constructed in 2 ways. A wide web aluminiumshoe with a broad toe that is available in sizes 00 to 5 isused as a template1. The basic shoe can be made from2 pieces of plywood. One piece of plywood is 0.64–0.95 cm thick and the second piece is 1.91 cm thick. Usingthe aluminium shoe as a template, the thinner piece ofplywood is cut out with a vertical border while the thickerpiece is cut out with the border bevelled at a 45° angleusing an angle saw2. As a modification to the basicpattern, the palmar or heel section of the wooden shoecan be cut at a 15, 30 or 45° angle or left straight if desired.The 2 pieces of plywood are glued together with thethinner portion proximal and two 2.54 cm drywall screws orwood screws are used to secure the 2 pieces together. Awood rasp or belt sander is used to blend the cut anglesinto a uniform slope (Figs 3a,b). Alternatively, the shoe canalso be fabricated from a single piece of 2.86 cm plywood(purchased as sub-flooring plywood) using the sametechnique as described above. Recently, one author (M.L.S.) has occasionallysubstituted ethyl vinyl acetate (EVA) for the thicker 1.91 cmsection of plywood and bevelled it in a similar manner. EVAis an extremely elastic material that can be sintered toform a porous material similar to rubber, yet with excellenttoughness. The compressibility and wearability of thismaterial allows 'selective' loading on the ground surfaceof the shoe which appears to further decrease the stresseson the lamellae and increase comfort (Fig 4). Additionallayers of plywood, rubber or EVA can be added toincrease the height of the wooden shoe when desired.Shoe height is dictated by the conformation of the hoofand the amount of displacement of the distal phalanxpresent; i.e. the greater the rotation of the distal phalanx,the more shoe height is necessary in order to achieve amore palmar placement of breakover. If the sole isprolapsed or the distal phalanx has penetrated the sole, arecess can be created in the dorsal surface of the shoe bycutting a half moon shape in the thinner piece of plywoodusing a router under the prolapsed tissue or a hand grindercan be used to create a trough in the shoe below thearea of the sole or bone that has prolapsed (Fig 5). The same end can be achieved by cutting the thinnerpiece of plywood or a leather pad in the shape of a 'W'and then attaching it to the thicker section of plywood asdescribed above (Fig 6). If heel elevation is required, the heels can be raised accordingly by applying a wedge padto the hoof surface of the wooden shoe. The angle of thewedge is usually 2–4° depending on the amount of heelhorn removed. The wedge pad is attached to the shoewith 2.54 cm drywall screws or wood screws. An alternativemethod to raise the heels is to cut the ground surface ofthe wooden shoe itself at an angle to the hoof surface. Application of the shoe A generalised outline will be used to describe thepreparation of the foot and application of the woodenshoe in horses with dorsal capsular rotation; bear in mindeach case of chronic laminitis must be treated on anindividual basis. The foot must be trimmed appropriately,and the shoe sized and positioned in relation to theunderlying distal phalanx regardless of the conformationof the hoof. Therefore, measurements must be made froma lateral radiograph taken prior to shoeing as a guide. Touse the radiograph for guidance, a vertical line is drawnfrom the center of rotation of the distal end of the secondphalanx to the ground. This line should correspond to thewidest part of the foot and can be used as a landmark onthe foot to begin the trim. Next a line is drawn parallel tothe solar border of the distal phalanx, starting 15 mm distalto the palmar process of the distal phalanx andcontinuing dorsally. The hoof wall to be removed in theheel area can be determined from the mass below thisline. A second line is drawn 15 mm dorsal and parallel tothe dorsal surface of the distal phalanx; this line is used toalign the dorsal hoof wall with the parietal surface of thedistal phalanx (Fig 7a,b) (Parks 2003; Parks and O'Grady2003; O'Grady 2006). The trim The initial step is to trim the heels and quarters of the wallas well as the angle of the sole to coincide with the first linedrawn on the radiograph. Any exfoliating horn is removedfrom the frog and the bars are trimmed on an angle towiden the sulci. If possible, the ideal end product is to havethe hoof wall at the heels and the frog trimmed so thatthey are on the same plane. This alone increases theground surface in the heel area and thus the ability toaccept load. If the foot can be trimmed to coincide withthe line drawn parallel to the solar surface of the distalphalanx, the palmar aspect of the ground surface of thefoot will be on a different plane to the dorsal aspect of theground surface, which will often unload the dorsal sectionof the foot. The dorsal hoof wall is trimmed to approximatethe line drawn parallel to the parietal surface of the distalphalanx to create a more acceptable alignmentbetween the dorsal hoof wall and the parietal surface ofthe distal phalanx. Following the trim, the foot is placed on the ground andthe horse is observed for any additional discomfort.Additionally, the horse is observed to see whether the heelof the foot is touching the ground at rest, and whether thehorse lands markedly toe first as it moves in a straight line. Ifany of these signs are present, heel elevation will benecessary to compensate for the increase in tension in thedeep digital flexor tendon caused by lowering the heels ofthe hoof capsule. Heel elevation is generally used if aflexural deformity involving the distal interphalangeal jointdescribed as phalangeal rotation is noted radiographically(O'Grady et al. 2007b). (Capsular rotation describes thedivergence of the dorsal hoof wall from the dorsal parietalsurface of the distal phalanx independent of therelationship of the distal phalanx with the phalangeal axiswhereas phalangeal rotation describes rotation of thedorsal surface of the distal phalanx palmarly/plantarly fromits normal orientation and relationship with the first andsecond phalanges.) The trim should never violate normalfarrier practices, such as invading sensitive tissue. Fitting the shoe A line is drawn across the widest part of the trimmed foot.Next, the foot surface of a wooden shoe is measured fromdorsal to palmar and then a line is drawn across themiddle of the shoe from lateral to medial. The correct sizeof the shoe is determined by superimposing the line drawnacross the foot and the line drawn on the shoe on top ofeach other; the appropriate size shoe will extend from theline drawn across the foot to the end of the heel or 0–8 mmpalmar to the heel. Using a 1.98 mm drill, a guide hole isdrilled through the lateral and medial side of the hoof wallat the widest part of the foot and 3.75 cm drywall screwsor wood screws are placed in each hole and screwed inuntil just visible on the ground surface. To recruit the sole,bars, frog and sulci for weightbearing, deformableimpression material3 is applied to the palmar/plantarsection of the foot of the foot.
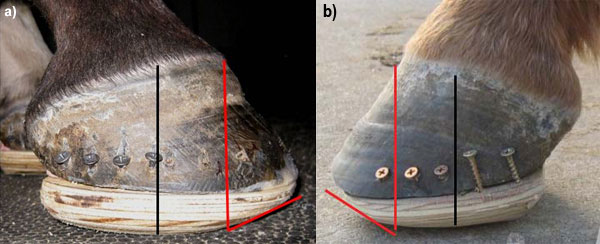
The shoe is now set in place on the ground surface ofthe foot and attached using the 2 dry wall screws or woodscrews. The foot is placed on the ground and allowed tobear weight in order for the impression material toconform between the palmar section of the foot and theshoe in the optimal form. Two or 3 more holes are drilledthrough both sides of the hoof wall and the shoe issecured in place using additional screws. These holes maybe predrilled from the solar surface of the foot if desired toensure accurate screw placement in the wall. If the massof the hoof wall is insufficient or if the quality of the hoofwall is insufficient to hold the screws, screws can beplaced in the wooden shoe against the outer surface ofthe hoof wall to act as struts and 5 cm casting tape4 isused to form an attachment between the hoof wall,screws and wooden shoe (Fig 8). With the foot on theground, a vertical line is drawn from the dorsal aspect ofthe coronary band to the ground. The point where the linemeets the ground is where the breakover point of theshoe should be positioned (Figs 9a,b,c). This point willusually be just dorsal to the dorsal limit of the solar margin of the distal phalanx. Setting the breakover to this point inthe shoe is easily accomplished using a hoof rasp with thefoot being held in the farrier position. Deep digitaltenotomy has been the recommended treatment whenpenetration of the distal phalanx through the sole hasoccurred secondary to dorsal capsular rotation. Oneauthor (S.E.O.) has observed that the wooden shoe hasprovided an alternative and often better means to treatthis condition without surgery.
Prolapse of the sole or penetration of the distal phalanx If the sole bulges distal to the level of the hoof wall or if the distal phalanx has penetrated the sole, the foot is trimmed to establish realignment, the wooden shoe is fitted to the trimmed foot and heel elevation is applied to the shoe to decrease the forces on the deep digital flexor tendon (Redden 1997). Before applying the shoe, the wooden shoe is placed against the solar surface of the foot and pressed against the sole or the exposed corium of the distal phalanx. The moisture of the tissue or a suitable dye applied to the corium will create an impression on the foot surface of the wooden shoe which can then be cut out using a router or a trough can be created with a grinder as illustrated in Figure 5. The shoe is now applied with screws and fibreglass tape, being sure that the impression material is concentrated palmar to the apex of the frog and not allowed to migrate dorsally. A window can be created in the fibreglass tape and the affected area can be packed with an appropriate antiseptic from the front of the shoe. Conclusions The authors have used the wooden shoe in their combinedpractices for the past 5 years and found this techniqueprovides another very consistent farriery option whentreating a horse with chronic laminitis. Removing the stresson the lamellae has always been difficult with traditionalshoes used to treat chronic laminitis as the shoe is placedunder the hoof wall concentrating the load on thecompromised lamellae. The solid plane of the woodenshoe, combined with the impression material allows loadsharing across the ground surface of the foot especially inthe palmar section of the foot and appears to decreasethe load borne by the hoof wall. This concept of loadsharing is very helpful in horses with foot conformation thathas limited hoof mass in the palmar section of the foot.Furthermore, cutting the perimeter of the wooden shoe ata 45° angle around the circumference of the foot isthought to decrease the lateral/medial torque on thelamellae especially when the horse turns (Steward 2003;O'Grady et al. 2007a). Therapeutic shoes used for treatingchronic laminitis are often deficient in providing sufficientbreakover and heel elevation due to the physical limits ofthe particular shoe whereas increasing the height of the wooden shoe allows the desired mechanics to befabricated into the shoe. Shoe height enhancesmechanical advantages as it allows dorsal breakover,lateral medial breakover and heel elevation to beincorporated into the shoe in a uniform manner. Creatinga recess in the shoe under the distal phalanx in the toearea relieves the load on dorsal aspect of the foot whilethe weightbearing function is concentrated in the palmarsection of the shoe. When displacement of the distalphalanx within the hoof capsule is severe, the woodenshoe seems to be an excellent method to act as atransient treatment to build sufficient hoof mass (wall andsole) to where a more conventional shoe can be appliedor the horse can remain barefoot. It should be noted thatthe heel elevation provided by the wooden shoe shouldnot be discontinued abruptly when this farriery method ischanged but rather decrease the heel elevationgradually over the next few months. Manufacturers' addresses
References
|