Farriery Options for Acute and Chronic LaminitisReprinted with permission from the American Association of Equine Practitioners. |
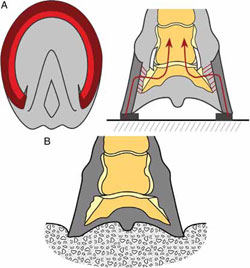 |
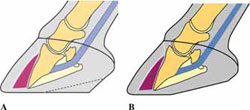
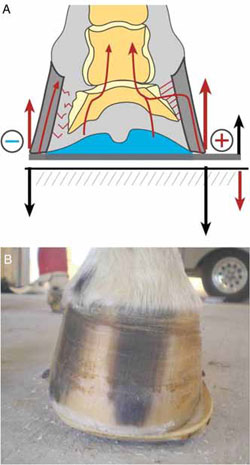
| Fig. 1. (A) Shows the load being placed directly on the lamellae when there is a shoe on the hoof or the horse is standing on a hard surface. (B) Shows the load being shared with structures on the ground surface of the foot when the horse is placed on a deformable surface or if a deformable material is placed on the ground surface of the foot. |
Three fundamental issues exist when presented with a patient with acute laminitis. The initial issue is that the examiner has no accurate means of knowing the extent of the laminar damage present and thus is unable to predict the future with reasonable accuracy. All cases of acute laminitis should be treated as an emergency and monitored closely.The number of horses that have suffered a severe episode of acute laminitis that are treated successfully is difficult to determine, but, in the authors' experience, this number is at best low to modest. The window of opportunity for treatment once clinical signs are apparent and a diagnosis has been made is relatively short. It is well known that the onset of cellular injury within the lamellae occurs during the developmental stage of laminitis and precedes the onset of pain and lameness. Cellular damage can exist for a period of time before the horse, owner, and veterinarian are aware that laminitis exists. Laminitis frequently stems from a systemic response to a disease process in an organ system remote from the foot such as the gastrointestinal, respiratory, reproductive, or endocrine systems. Therefore, medical treatment during the acute stage needs to aggressively address the initiating cause of laminitis or if treatment of the cause was initiated before the onset of laminitis, it should be continued.
Second, there is no practical means to counteract the vertical load of the horse's weight that is placed on its feet.2 The mass of the horse can only be slightly altered, and no method of so-called foot support will alter the vertical load. If the horse is shod or if the horse stands on a hard surface, weightbearing is concentrated around the perimeter of the hoof onto the compromised lamellae. In acute laminitis, it may be appropriate to remove the shoes if shod and apply some type of deformable material to the solar surface of the foot such that the sole, bars,and frog in the palmar/plantar section of the foot become load sharing with the hoof wall (Fig. 1, A and B). Frog support by itself has become ingrained in the veterinary and farrier literature as such a method to support the weight of the horse. The anatomy of the bottom of the horses' foot is such that the horny frog (which varies in thickness) and the digital cushion above it are both readily compressible structures under pressure. When pressure is placed over the frog, it quickly deforms and is compressed,and the interface between the ground surface of the frog and the solar surface of the distal phalanx (P3) is diminished. The frog can be irreversibly damaged by applying this focal pressure,and in some horses, it can and will cause increased pain/lameness.a It is the author's belief that frog support alone is not beneficial. In the author's experience,it is more advantageous to recruit the entire solar surface in an attempt to reduce the mechanical stresses on the lamellae. This can be accomplished by applying either thick styrofoam,one of the deformable silicone impression materials,or removable boots that contain an insert, or by placing the horse in sand. It should be noted that when using sand, "beach" sand rather than construction sand is preferable because of its ability to conform to the bearing surface of the feet and not pack. Applying shoes in the acute stage of laminitis has not been shown to offer any advantages.
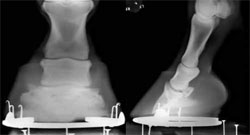 |
| Fig. 2. Radiographs illustrate severe distal displacement of the distal phalanx 7 days after showing the onset of acute laminitis. |
The third factor is the distractive forces on the lamellae caused by the moment about the distal interphalangeal joint associated with tension in the deep digital flexor tendon (DDFT). In the acute stage, this can be countered to some extent by providing mild heel elevation and by moving the breakover in a palmar/plantar direction. Raising the heels excessively in the acute stage has been advocated by some, but in our experience should be done with caution because there is no factual evidence to substantiate a beneficial effect.1
Distal displacement (sinking) of the distal phalanx occurs when the entire lamina attachments are sufficiently damaged allowing the distal phalanx to displace uniformly within the hoof capsule (Fig. 2).There is minimal involvement of the DDFT during the process of distal displacement. A common treatment regimen for distal displacement is to raise the heels with the theory that it decreases stresses on the DDFT; a practice that the authors have not seen to be successful. Moving the breakover back and placing a uniform layer of a deformable impression material on the bottom of the foot or placing the horse in sand are preferable in the authors' experience;however, patients with severe distal displacement carry a reasonably poor to grave prognosis.
Recently, one author (SOG) has applied wooden shoes, which have the perimeter of the ground surface of the shoe at the toe and sides cut on an angle, to a limited number of horses with acute laminitis that are expected to rotate or sink, and the results have been very encouraging. In theory, this shoe would seem to primarily redistribute the weight while reducing the torque on the lamellae around the entire circumference of the foot.
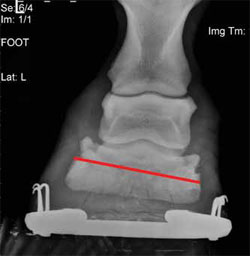 |
| Fig. 3. Radiograph of asymmetrical downward displacement of the distal phalanx on the medial side. Note a line drawn through the solar foramens is not parallel with the ground. Also note the disparity in the joint space from the lateral to the medial side. |
 |
| Fig. 4. The red arrow shows the position of the breakover after a bevel has been created in the ground surface of the dorsal hoof wall. |
Radiology
The lateral radiograph has always been considered the "gold" standard for evaluating acute and chronic laminitis, but it limits the evaluation of the distal phalanx to one plane. It does not allow identification of asymmetrical medial or lateral distal displacement of the distal phalanx. Therefore, the authors consider it crucial that a dorsopalmar (dorso 0° palmar) radiographic projection be included as part of the radiographic study for either acute or chronic laminitis.3 Quality radiographs are needed to visualize the osseous structures within the hoof capsule and the hoof capsule itself. Radio-opaque markers can be used to determine the position of the distal phalanx in relation to surface landmarks.
Baseline radiographs should be taken in the acute stage of laminitis and can aid the diagnosis by measuring the distance between the outer hoof wall and the parietal surface of the distal phalanx, as well as assessing hoof capsule conformation to determine whether trimming changes are necessary.
The radiographic features of chronic laminitis are well documented.4 The following observations from the lateral radiograph are important in determining the prognosis and guiding treatment: the thickness of the dorsal hoof wall, the degree of dorsal capsular rotation, the angle of the solar surface of the distal phalanx relative to the ground, the distance between the dorsal margin of the distal phalanx and the ground, and the thickness of the sole.
The dorsopalmar radiograph is examined to determine the horizontal position of the distal phalanx in the frontal plane. Asymmetrical distal displacement of the distal phalanx on either the lateral or medial side is present if an imaginary line drawn across the articular surface of the distal interphalangeal joint or between the solar foramens of the distal phalanx is not parallel to the ground, the joint space is widened on the affected side and narrowed on the opposite side, and the width of the hoof wall appears thicker than normal on the affected side. If the position of the coronary band is visible on the radiograph, the distance between the coronary band and the palmar processes of the distal phalanx will be greater on the affected than the unaffected side (Fig. 3).3
With the advent of digital radiography, an image can be generated on site during the initial examination of either acute or chronic laminitis.
Farriery in the Acute Stage
Examination of the foot during acute laminitis should evaluate the digital pulse, the coronary band, hoof capsule, and the integrity of structures of the hoof capsule. Special attention should be directed to those structures in the palmar/plantar section of the foot that will be used for support. If the heels of the hoof capsule are damaged or poorly conformed and the frog and digital cushion lack mass, it may be difficult to use these weakened or damaged structures for support. Hoof tester examination is useful in determining both the presence and absence of pain, as well as providing the examiner with more information regarding the strength and integrity of the structures tested. If the horse is shod, the shoes are removed as a traumatically as possible. If the foot is overgrown or neglected, it is trimmed in such a manner that will concentrate the load under the foot. This trimming is done using radiographic guidance whenever possible. Every effort is made to preserve the depth of the dorsal half of the sole. When extensive trimming is unnecessary, the author will gently rasp the heels from the widest part of the foot palmarly/plantarly just to the point where the heels of the hoof wall and frog are aligned on the same plane. Excessive lowering of the heels in the acute stage can be harmful. The sole dorsal to the frog is evaluated for depth by radiology and by using digital pressure either by hand or whether it deforms when pressure is applied with hoof testers. If the sole has adequate depth, a rasp is placed across the foot from quarter to quarter such that the apex of the frog is centered in the middle of the rasp. Using the leading edge of the rasp, a line is drawn across the solar surface of the foot with a marker. The rasp is used to bevel the foot in a dorsal direction from this line forward. This effectively moves the breakover palmarly, decreases the moment on the dorsal lamellae, and may lessen the forces on the lamellae created by the DDFT (Fig. 4).
Various methods of foot support have been advocated and are in routine use. These include thick soft bandages, thick styrofoam, deformable silicone impression material,b numerous commercial pads, commercial boots with a deformable insert,c and sand. The chosen method or combination of methods is based on familiarity, preference, availability, owner compliance, cost, and the foot conformation to which it is to be applied. Whatever method is chosen, it should encompass all the structures in the palmar/plantar section of the foot instead of relying on the frog alone. Excess pressure placed solely on the frog or on weak structures in the heel area of the hoof capsule over time may further and negatively alter these structures and thus reduce mass. Heel elevation if desired can be accomplished using any of the above methods. Absolute stall rest in acute laminitis is imperative because movement of the horse is associated with increased stress within the damaged lamellae.
Chronic Laminitis
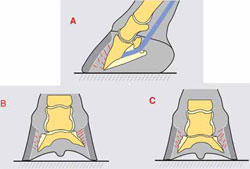 |
| Fig. 5. (A) Illustrates dorsal capsular rotation, (B) illustrates mediolateral rotation and (C) illustrates distal displacement. |
Chronic laminitis is defined by the presence of mechanical collapse of the lamellae and displacement of the distal phalanx within the hoof capsule.5 There are three manifestations of displacement of the distal phalanx: dorsal capsular rotation, distal displacement (sinking), and mediolateral rotation or asymmetrical distal displacement. A combination of all three forms of displacement can exist simultaneously (Fig. 5). Lamellar separation of the distal phalanx occurs when the forces in the lamellae exceed their tensile strength. In simplistic terms, the acute phase is the phase of injury and chronic phases are phases of tissue repair. The eventual outcome of the treatment for horses with chronic laminitis can be divided into function and morphology.The functional outcome is most likely to dictate the difference between athletic performance,pasture soundness, and euthanasia. The morphologic outcome is more likely to determine the degree to which continued and potentially lifelong corrective measures are necessary. At the onset of chronic laminitis, the eventual outcome is hard to predict, but the most important indicator for survival remains the severity of the initial insult to the lamellae. The appearance of the initial radiographs does not necessarily correlate with either the functional or morphologic outcome. The thickness of the sole and the angle between the solar surface of the distal phalanx and the ground seem to be better indicators of the difficulty of treatment of horses with dorsal phalangeal rotation, and both of the separameters are more useful than the degree of capsular rotation in successfully predicting the rehabilitation of the horse.6 In contrast to treating horses with acute laminitis, in which medical therapy frequently assumes priority, supportive therapy or hoof care is the most important element for success in treating horses with chronic laminitis.
Farriery in the Chronic Stage
The mainstay of hoof care is therapeutic trimming/shoeing. In considering hoof care in horses with chronic laminitis, there are three goals for therapy: to stabilize the distal phalanx within the hoof capsule, to control pain, and to encourage new hoof growth to assume the most normal relationship to the distal phalanx possible.3,6
Attempting to stabilize the distal phalanx within the hoof capsule is important to prevent further rotation/displacement, promote healing, and decrease pain. Therefore, understanding how the stability of the distal phalanx within the hoof capsule affects the rehabilitation of a chronically laminitic horse is crucial to a successful outcome. The best indication available that the distal phalanx is more stable is that the horse is more comfortable because increased stability decreases tissue trauma.
To achieve the goals outlined above, there are several farriery principles or objectives that must be followed. Stabilizing the hoof capsule requires decreasing the stress on the most damaged lamellae. Therefore, the objectives are to reduce the load on the most severely affected wall and transfer load to less severely affected wall, recruit all available ground surface of the foot to bear weight, and decrease the moment about the distal interphalangeal joint as necessary. To summarize these principles in simplistic farriery terms: (1) recruit all available ground surface that is capable of bearing weight, (2) position breakover appropriately, and (3) provide heel elevation if necessary. Pain caused by lamellar stress and injury is in part controlled by increasing stability within the foot. An important objective is limiting the residual capsular rotation as the hoof grows to eliminate load on the affected section of the foot. There are a limited, although steadily increasing, number of methods and materials available to the veterinarian and farrier to apply these principles, but the variety of ways in which they can be applied is even greater. Above all, focus should be maintained on principles and not methods.
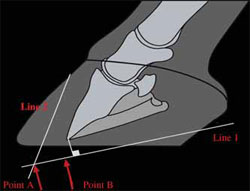 |
| Fig. 6. A schematic representation of a lateral radiograph of a foot with dorsal capsular rotation. Line 1 is drawn approximately parallel and about 15 mm distal to the solar surface of the distal phalanx. Line 2 is drawn parallel and approximately 15-18 mm dorsal to the parietal surface of the distal phalanx. Point A at the intersection of line 1 and line 2 is the furthest dorsal point the toe of the shoe should be set. Point B is approximately 6 mm dorsal to the dorsal margin of the distal phalanx and is the approximate location of the point of breakover. |
 |
| Fig. 7. (A) A schematic diagram of a horse's foot with chronic laminitis that has recently developed severe dorsal capsular and phalangeal rotation. (B) After trimming along line 1 in figure 6. Note that the dorsal and palmar aspects of the ground surface now form 2 different planes. |
The Trim
The trim is the basis for treatment of all horses with chronic dorsal capsular/phalangeal rotation. Trimming a horse is usually performed using guidelines based on anatomical landmarks derived from the exterior surface of the hoof capsule. These landmarks reflect the position of the underlying distal phalanx. The external landmarks of the hoof capsule on a horse with laminitis may no longer reflect the underlying position of the distal phalanx because the distal phalanx has moved relative to the capsule and the growth pattern of the hoof capsule changes. The immediate objective of the trim is to re-align the ground surface of the hoof capsule with the solar margin of the distal phalanx.3,6-8 To do this accurately and consistently requires radiographic guidance.
The plane of the trim can be estimated from the radiograph by drawing a line approximately parallel to and 15-20 mm distal to the solar margin of the distal phalanx and trimmed accordingly (Fig. 6). Depending on the degree of rotation and the amount of sole growth after the injury, the distance from the dorsal margin of the distal phalanx and the ground surface is frequently less than the desired depth. However, in horses in which the dorsal sole is <15-20 mm, the ground surface of the hoof cannot be re-aligned to the solar margin of the distal phalanx from the toe to the heels without reducing the thickness of the sole. Therefore, in those horses, the walls and sole can only be trimmed palmar to the point where the distance between the solar margin and the ground surface of the hoof capsule is >15-20 mm. Consequently, the dorsal and palmar aspects of the ground surface of the hoof capsule may form two different planes after being trimmed (Fig. 7, A and B). The other consequence of trimming the foot in this manner is that lowering the heels causes increased tension in the deep digital flexor tendon, which may increase the pain associated with weight bearing and movement. Both the uneven ground surface and the increase in deep digital flexor tendon tension should be addressed at the time of shoeing.
Realignment of the distal phalanx in a dorsopalmar plane as described for dorsal capsular rotation is not applicable for distal displacement or mediolateral displacement, so trimming is seldom necessary.
Some horses may be satisfactorily treated with trimming alone because they often have minimal rotation, sufficient sole depth, and are comfortable walking on soft surfaces with or without low doses of analgesics. Boots with foam pad insertsc may be used to make barefooted horses more comfortable.
Shoeing
It is readily apparent that no single prescription, shoe type, or device is consistently effective in treating horses with chronic capsular and/or phalangeal rotation. However, the authors use the following guidelines that seem useful and can be adapted to the needs of the individual horse.
General Guidelines for Shoeing Horses With Dorsal Capsular Rotation
There are three main considerations involved in shoe selection and shoeing technique: (1) where to position the point of breakover; (2) whether to provide support for the ground surface of the frog and sole, and if so which type; and (3) whether to elevate the heels. The objective of moving the point of breakover palmarly is to improve the ease of movement by decreasing the stresses within the dorsal lamellae. There is some debate as to what the optimal position for the point of breakover should really be in horses with dorsal capsular rotation. However, a good guideline is to draw a line on the radiograph from the dorsal margin of the distal phalanx to the line indicating the desired plane of the trim and perpendicular to it (Fig. 6). The point of breakover is positioned ~6-9 mm dorsal to the junction of the two lines. Some clinicians will position the point of breakover palmar to the dorsal margin of the distal phalanx but this can significantly decrease the amount of weight-bearing ground surface of the foot. Additionally, positioning of the dorsal margin of the shoe warrants attention. The most dorsal point where the shoe should be positioned is best determined by drawing a third line on the radiograph, parallel and ~15-18 mm from the parietal surface of the distal phalanx (Fig. 6). The dorsal margin of the shoe should be positioned no further dorsally than the intersection of this line and the line indicating the ideal plane of the ground surface of the foot (Fig. 6). If it is positioned dorsal to this point and contacts the dorsal hoof wall, it may cause excessive tension in the dorsal lamellae and cause distortion of future growth of the dorsal wall, resulting in being directed away from the parietal surface of the distal phalanx. The position of the point of breakover can be moved palmarly to the dorsal margin of the hoof by rolling the toe, squaring the toe, or using a hand grinder to create the desired breakover in the toe of any shoe.
The objective of elevating the heels is to decrease the tension in the DDFT, which decreases the moment about the distal interphalangeal joint with the intention of decreasing the stresses within the dorsal lamellae. This is usually most appropriate in horses with phalangeal rotation that are landing toe first. The amount of heel elevation in the authors' opinion varies between 2° and 4°. Heel elevation may be obtained with wedged shoes, bar wedge inserts, or rails (described below). The efficacy of heel elevation is best judged by the comfort of the horse, after trimming at rest and walking. How a horse lands is a good guideline that the amount of heel elevation is appropriate. Ideally, the heel elevation is such that the horse just lands heel first. If a horse lands markedly heel first, there is too much heel elevation, and if it lands toe first, there is not enough heel elevation. This assumes that other causes of pain have been precluded, particularly dorsal sole pressure. Unfortunately, prolonged heel elevation may result in heel contracture, which potentially causes the heels themselves to become painful. Thus, it is prudent, if using heel elevation, to remove it as rapidly as possible compatible with the improvement in lameness.
How aggressive to be in using these principles depend on the amount of displacement and the response to therapy. An experienced clinician may well have a good idea when and how to apply anyone or all of these principles based on history, physical examination, and radiographs.
Types of Shoes
Similar results may be obtained with several, if not many, different methods of shoeing. Success with any given technique increases with the experience of both the veterinarian and the farrier. Therefore, all of the following have merits, and all have had their successes and failures.6 The authors have the most experience and have had reasonable success using the wide web aluminum rail shoe and the wooden shoe.3,5,10 The merits of each type of shoe are described below.
Egg-Bar Shoe
The egg-bar shoe is a closed heel shoe in which the bar extends palmarly. This palmar extension may function as a lever if the shoe extends too far beyond the heels. Specifically, if the horse is kept on deep soft bedding, it causes the heels to remain higher on the bedding than the toe and can function as a heel wedge. The toe of the shoe may be squared, rolled, or moved palmarly to position the point of breakover appropriately. In horses with chronic laminitis, egg-bar shoes should be used in conjunction with a synthetic polymer to provide support to the ground surface of the foot depending on the degree of stability of the distal phalanx. Additional heel elevation may be obtained by using a wedged rim pad or a manufactured wedge shoe. The disadvantage to this shoe is that it does not ease mediolateral breakover.
Heart-Bar Shoe
The heart-bar shoe should be positioned in relation to the solar margin of the distal phalanx as previously described. Its toe can be squared, rolled, or moved palmarly to position the point of breakover appropriately. Guidelines usually cited suggest that the apex of the bar should extend to a point 9 mm palmar to the trimmed apex of the frog. The heart-bar is thought to enable the frog to load and redistribute some of the weight born by the limb away from the wall. It is unknown if the heart-bar shoe provides any other benefit. Heart-bars are frequently welded into an egg-bar shoe commonly referred to as a full support shoe. This provides the added benefit of functioning like a wedge as previously described. Also, heart-bar shoes are increasingly used in combination with other forms of sole support that are either poured or pressed into the cavity formed between the branches of the shoe and the bar to provide additional support to the ground surface of the foot. Disadvantages of this shoe are that its application demands skill, it is difficult to apply heel elevation, and again, the shoe does not address mediolateral breakover.
Reverse Shoe
The principle benefits of a reverse shoe are that it moves the breakover palmarly because the toe of the shoe is absent, it puts no pressure on the dorsal sole, and it functions as an egg-bar shoe at the heels. Depending on the degree of stability within the foot, it must be used with appropriate sole and frog support. The principle disadvantage of this style of shoeing is that it concentrates stress where the dorsal margins of the branches of the shoe contact the wall. This shoe is most useful in horses in which there is a wound on the dorsal aspect of the sole that requires treatment and would be covered up by the toe of other shoe types. Furthermore, it does not ease mediolateral breakover.
 |
| Fig. 8. A wide web aluminum shoe with rails welded on the branches. |
 |
| Fig. 9. The basic wooden shoe where the proximal piece is cut vertical and the thicker piece is cut on a 45 degree angle. Note the wedge pad attached to the wooden shoe for heel elevation if necessary. |
 |
| Fig. 10. A wooden shoe applied to the foot with impression material. Black arrow is the widest part of the foot. Red line denotes the point of breakover on the ground surface of the shoe. |
 |
| Fig. 11. (A) Schematic illustration that shows the forces being moved away from the medial displacement toward the good side of the foot. (B) Wooden shoe shoeing extension. Note the disparity of the growth rings at the coronet with no growth present on the side with displacement. |
Wide Web Aluminum Rail Shoe
Wide web aluminum rail shoes are based on an open heeled pattern with square, blunt, or heavily rolled toes. This type of shoe makes use of "rails." Rails are narrow, wedge-shaped distal extensions that are applied to the axial side of the ground surface of the shoe. As such, they elevate the heels and ease medial and lateral breakover (Fig. 8). A commercial shoeing systemd provides a wide web aluminum shoe where the rails can be bolted onto the shoe; otherwise, the rails are machined into or welded onto or glued onto the aluminum rail shoe. The rails can be made in different heights. The advantage of the commercial system is that the rails can be changed to alter the height after the shoe has been applied to the horse's foot. Both shoes are used in conjunction with sole and frog support. When using the aluminum rail shoe, the sole and frog support is achieved by applying silicone putty between the branches of the shoe. The shoe provides improved breakover, heel elevation, and sole and frog support. The wide web aluminum shoe can also be used with a 2° or 3° bar wedge substituted for the rails. In this case, the lateral and medial quarters of the shoe are beveled substantially with a grinder for breakover. In fact, this bevel can be incorporated into the branches of the lateral and medial quarters of any shoe.
Wooden Shoe
The wooden shoe is generally fabricated from plywood. It is shaped based either on the natural shape of the foot or the closest fitting Natural Balancee shoe. The principle layer is cut out of 3/4-in plywood, and the perimeter is beveled at an angle of 45°. This not only moves the breakover palmarly but also moves the medial and lateral weight-bearing surfaces axially enhancing medial and lateral breakover (Fig. 9). Two main modifications of this pattern have been described. In one, a second layer of 3/4-in thick rubber matting, cut to match the ground surface of the block, is screwed to the ground surface of the shoe. The margins of the rubber are beveled in a similar manner to the wood to further enhance breakover. In the second modification, a second layer of 1/2- or 3/8-in plywood is cut to match the foot side of the shoe and attached to it with glue and screws.3,10 The bevel on the front of the shoe is then increased with a rasp until the point of breakover is positioned to correspond to vertical line drawn from the coronary band (Fig. 10). A layer of silicone putty is applied between the ground surface of the foot and shoe and allowed to set with the horse in a weight-bearing position. The shoe is attached with screws inserted through pilot holes drilled in the distal hoof wall and into the shoe. Alternatively, screws can be screwed into the plywood adjacent to the margin of the distal hoof wall and the shoe secured by incorporating the screw heads in a synthetic adhesive applied to the adjacent wall or by placing 2-in casting tape around the perimeter of the foot. A wedge pad may be applied to the foot surface of the shoe to provide heel elevation if needed. If the sole has prolapsed below the level of the wall or if the distal phalanx has penetrated the sole, the foot surface of the shoe is recessed to remove any direct pressure from the sole and the silicone putty removed from that area.
Mediolateral Rotation of the Distal Phalanx
As a much less recognized condition than dorsal capsular rotation or distal displacement, less is known about treating horses with mediolateral rotation of the distal phalanx. Theoretically, the hoof capsule can be stabilized in relation to the distal phalanx by reducing the weight bearing on the affected side by increasing weight bearing on the contralateral side. This is best accomplished by extending the shoe on the contralateral side to act as a lever and hence acts as a mild wedge.3 The authors have had success in controlling mediolateral rotation in a limited number of horses by applying either the rail shoe or the wooden shoe in combination with silicone putty and setting the shoe wide on the unaffected side (Fig. 11). This has visibly improved comfort, promoted hoof wall growth at the coronet on the affected side, and/or abolished the evidence of mediolateral rotation over time. This technique seems promising, but because the complication rate with this condition seems to be high, the prognosis for treating this pattern of displacement is still less favorable than it is with dorsal capsular/phalangeal rotation.
Conclusions
Unfortunately, all of the treatment regimens, both medical and farrier techniques, used to treat acute and chronic laminitis are based on tradition, theoretical assumptions that a given treatment should work, and anecdotal evidence that a certain type of treatment has worked on previous cases. There are limited controlled studies comparing efficacy of the numerous treatments in use and there is no scientific proof that one treatment is superior to another.11,12 What are well documented are the forces and mechanics applicable to the equine foot. As clinicians (veterinarians and farriers), we may be better served by a thorough knowledge and understanding of the anatomy, physiology, and function of the hoof. Understanding the foot in a mechanical sense may allow us to better apply our preferential treatment.
Treatment of laminitis must be a group effort equally shared between veterinarian, farrier, and owner. The intent of this paper is not to discourage treatment of laminitis but to create expectations that are realistic, humane, and based on the cause of the disease, degree of lamellar damage, pain, duration, and the financial constraints involved in prolonged treatment. At the onset of treating chronic laminitis, certain guidelines should be outlined to indicate the efficacy of the chosen treatment method along with a reasonable timeframe for improvement. These guidelines could be a change in stance, decreased digital pulse, increased comfort, horn growth at the coronet, sole growth, etc. If the desired improvement is not observed or the condition gets worse, the overall farriery methods should be reassessed and changed where necessary.
For horses with severe laminitis, it is often impossible to rehabilitate them to the point where they have an acceptable quality of life. The main reason is that there are insufficient lamellae remaining within the hoof capsule to achieve stability and realignment. It is important from a humane perspective to know when to discontinue treatment that has not been effective. Often we persevere with various treatments and put the horse through much unnecessary suffering only to achieve an unsatisfactory outcome.
References and Footnotes