Acute and Chronic Laminitis: an OverviewIndividualized approach based on adherence to principles produces best resultsReprinted with permission from the American Farrier Journal. |
 |
| FIGURE 1.The arrow denotes the point of breakover after the toe has been beveled on the ground surface. |
 |
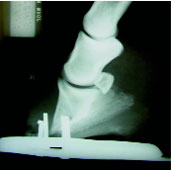
| FIGURE 2. Lateral and dorsopalmar radiographs of a horse with severe distal displacement taken 10 days after the onset of symptoms. |
 |
| FIGURE 3. A dorsopalmar radiograph showing displacement of the distal phalanx in a horizontal plane. |
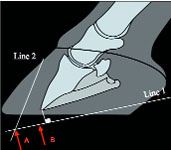 |
| FIGURE 4. A schematic drawing of a radiograph used for realignment of distal phalanx. It shows the lines drawn parallel to the solar surface of the distal phalanx (Line 1) and the line drawn parallel to the dorsal surface of the distal phalanx as well as the desired position of the point of breakover (Point B). |
2. We have no practical means to counteract the vertical load of the horse's weight that is placed on its feet. In other words, we have no method that allows us to take weight off the inflamed lamellae.If the horse is shod or if the horse stands on a hard surface, weight bearing is transferred from the perimeter of the hoofwall onto the compromised lamellae.
In acute laminitis, it may be appropriate to remove the shoes if the horse is shod and apply some type of deformable material to the solar surface of the foot such that the sole, bars and frog in the palmar/plantar section of the foot become load sharing with the hoof wall. Frog pressure has become ingrained in the veterinary and farrier literature as a method to support the weight of the horse. The anatomy of the bottom of the horses' foot, the horny frog (which varies in thickness) and the digital cushion above it, both are readily compressible structures under pressure.
When pressure is placed over the frog, it quickly deforms, compresses and the interface between the outer surface of the frog and the solar surface of the distal phalanx (P3) is diminished. These structures can be irreversibly damaged by frog pressure and the animal will often feel more discomfort. To counteract the forces acting on the bottom of the foot,it may be more advantageous to recruit the entire solar surface of the foot instead of relying on one structure.
This can be accomplished by applying either thick styrofoam, one of the deformable impression materials or placing the horse in sand. Applying shoes in the acute stage of laminitis, in my opinion, has not been shown to offer any advantages.
3. The distractive force placed on the lamellae by the deep digital flexor tendon (DDFT). In the acute stage this can be decreased to some extent by moving the breakover in a palmar /plantar direction.A line is drawn across the solar surface of the foot dorsal to the frog and a rasp is used to bevel the foot in a dorsal direction from this line. This effectively moves the breakover palmarly, decreases the moment on the dorsal lamellae and may lessen the forces created by the DDFT (Figure 1). Raising the heels excessively in the acute stage has been advocated by some but should be done with caution, as there is no scientific proof of a beneficial effect.
Laminitis as a consequence of systemic disease such as gastrointestinal problems, respiratory disease, retained fetal membranes or contralateral limb laminitis results in distal displacement(sinking) of the distal phalanx ( Figure 2).In this case the entire lamellae attachments are damaged, allowing the distal phalanx to sink uniformly within the hoof capsule.
Raising The Heels
There is minimal involvement of the deep digital flexor tendon during this sinking process. A common treatment regimen for distal displacement is to raise the heels with the theory that it decreases stresses on the DDFT, a practice that I have not seen to be successful. Moving the breakover back and placing a uniform layer of a deformable impression material on the bottom of the foot or placing the horse in sand may be a better option.
Recently, I have applied wooden shoes to horses with acute laminitis that are expected to rotate or sink. These shoes have the border of the ground surface at the toe and sides cut on an angle and the results are very encouraging. They will be described later in the text.
Baseline radiographs consisting of a lateral and dorsopalmar view (to diagnose unilateral displacement of the distal phalanx in a horizontal direction) should always be taken during the initial examination of acute laminitis. They can be used to determine previous damage, to follow the progression of the disease and as a guide to trimming and shoeing the horse at the appropriate time.
Chronic Laminitis
Rehabilitation of the horse with chronic laminitis is not a “cookbook” process as affected horses with chronic laminitis will vary from horse to horse and foot to foot and our understanding of the disease is still vague. However, the understanding of digital mechanics has improved and technological advances in shoe design and materials and techniques continue to expand.
Chronic laminitis by definition means that the distal phalanx (P3) has displaced within the hoof capsule. The distal phalanx can rotate downward at the toe,rotate to either side (laterally or medially) or it can totally displace (sink) within the hoof capsule. Rehabilitation of the horse with chronic laminitis will again depend on the amount of viable lamellae that remain intact, the conformation of the foot and the ability to realign the distal phalanx within the hoof capsule.
The question is often asked as to when a horse with chronic laminitis should be shod. The guidelines are:
I have never been successful nor have I observed improvement in the laminitic state when having to use local anesthesia in order to lift the horses foot and apply a shoe before the foot has stabilized.
Radiology
The lateral radiograph is often the only film taken for evaluating chronic laminitis but it does not allow identification of asymmetrical medial or lateral distal displacement. Therefore, the author considers it crucial that a dorsopalmar (AP) radiographic projection is included as part of the radiographic study for either acute or chronic laminitis. High quality radiographs are required to visualize the osseous structures within the hoof capsule as well as the hoof capsule itself.
Radio-opaque markers can be used to determine the position of the distal phalanx in relation to surface landmarks.The radiographic features of chronic laminitis are well documented.
The following observations from the lateral radiograph are important in determining the prognosis and guiding treatment:
The dorsopalmar radiograph is examined to determine the position of the distal phalanx in the frontal plane.Asymmetrical distal displacement of the distal phalanx on either the lateral or medial side is present if an imaginary line drawn across the articular surface of the distal interphalangeal joint or between the solar foramens of the distal phalanx is not parallel to the ground, the joint space is widened on the affected side and narrowed on the opposite side,and the width of the hoof wall appears thicker than normal on the affected side (Figure 3).
Finally, radiology will form the guidelines to be used in realigning the distal phalanx and applying any type of farriery (Figure 4).
Farriery
Trimming and shoeing has always been the mainstay of treating chronic laminitis and is directed at reducing andor removing the adverse forces on the compromised lamellae. In considering hoof care in horses with chronic laminitis, there are three goals for therapy:
Realignment of the third phalanx to create a better relationship of the solar surface of the distal phalanx with the ground is used as the basis for treating chronic laminitis. Realignment of the distal phalanx should promote and produce hoof wall growth at the coronet and sole growth under the distal phalanx.
Applying any type of shoe following this procedure should complement the realignment of the distal phalanx and further decrease the forces on the lamellae.
The principles applied to all shoeing methods used in treating chronic laminitis are to recruit ground surface, reposition the breakover palmarly and to provide heel elevation as needed. Our shoe of choice is usually some type of wide web aluminum shoe with heel elevation either incorporated within the shoe, in the form of rails or a heel wedge insert if an adequate heel base is present.
Deformable impression material is applied between the branches of the shoe to increase the surface area and redistribute the load. Breakover can easily be cut into the shoe in the appropriate place using a grinder. The center of rotation can be used for accurate placement of the shoe on the foot.
 |
| FIGURE 5.This is a wooden shoe with impression material. The black arrow signifies the widest part of the foot. Red line denotes the point of breakover on the ground surface of the shoe. |
 |
| FIGURE 6. A wooden shoe applied to the foot with screws placed against the foot at the heels to act as struts to accommodate fiberglass-casting tape. |
Recently this writer has been very successful using a wooden block cut in the shape of the foot with the border of the ground surface cut on an angle of at least 45 degrees (Figure 5). The foot is trimmed appropriately to address realignment, impression material is formed to create an interface between the solar surface of the foot and the wooden shoe, heel elevation is used if necessary and the shoe is applied atraumatically using screws, casting tape and or a composite (Figure 6).
With this procedure flat, even pressure is placed across the palmar section of the foot and all the mechanics are placed in the block while preserving the hoof capsule.
Surgery
Deep digital flexor tenotomy remains a very useful procedure for treating chronic laminitis. I consider this surgery necessary if the margin of the distal phalanx has prolapsed through the sole or on those cases that fail to stabilize once they begin displacing.
As stated earlier, two of the main detriments when treating chronic laminitis are the weight of the horse and the distractive force of the DDFT. One of these detrimental forces can be removed through this surgery. but knowing when to use it may pose a dilemma. It is often necessary to use this procedure in order to realign the distal phalanx.
 |
| FIGURE 7. A radiograph showing marked rotation with a flexural deformity involving the DIP joint. A DDF tenotomy is necessary to realign the distal phalanx. |
Further indications for this surgery are progressive rotation, persistent pain,minimal hoof wall and/or sole growth and secondary flexor apparatus contracture.If a marked flexural deformity involving the distal interphalangeal joint (DIP) is present, this is an indication of shortening of the musculotendonous unit and a release procedure is necessary to accomplish realignment of the distal phalanx (Figure 7).
It has to be emphasized that if a deep digital flexor tenotomy is utilized, it must be accompanied by realignment of the distal phalanx to decrease the adverse forces on the lamellae. Following a DDFT tenotomy, the second phalanx will move distal and palmarly relative to the distal phalanx (P3). This concentrates the load on the palmar soft tissue structures of the foot rather than redistributing the load on the solar surface of the distal phalanx.
The author has found it helpful to use a shoe or a cuff to extend the ground surface beyond the heel and add a few degrees of heel elevation. This will realign the digital axis and appears to improve the clinical perimeters (comfort, hoof capsule changes, sole growth, etc.) following surgery.
Perspective
Unfortunately, many of the treatment regimens — both medical and farriery —that are used to treat acute and chronic laminitis are based on tradition, theoretical assumptions that a given treatment should work and anecdotal evidence that a certain type of treatment has worked on previous cases.
There are no controlled studies comparing efficacy of the numerous treatments in use nor is there any scientific proof that one treatment is superior to another. What are well documented are the forces and mechanics applicable to the equine foot. As clinicians (veterinarians and farriers), we may be better served by a thorough knowledge and understanding of the anatomy, physiology and function of the hoof.Understanding the foot in a mechanical sense may allow us to better apply our preferential treatment.
Treatment of laminitis has to be a group effort equally shared between veterinarian, farrier and owner. The intent of this paper is not to discourage treatment of laminitis but to create expectations that are realistic, humane and based on the cause of the disease, amount of lamellar damage, pain, duration and the financial constraints involved in prolonged treatment.
Establishing Guidelines
At the onset of treating chronic laminitis, certain guidelines should be outlined to indicate the efficacy of the chosen treatment method along with a reasonable timeframe for improvement.
These guidelines could be a change instance, decreased digital pulse, increased comfort, horn growth at the coronet, sole growth, etc. If the desired improvement is not observed or the condition gets worse, the overall farriery methods should be reassessed and changed where necessary.
With severe laminitis cases, we are often unable to rehabilitate the horse to where it has an acceptable quality of life.The main reason being that there are insufficient soft tissue structures remaining within the hoof to achieve realignment.
I think it is important from a humane perspective to know when to discontinue treatment that has not been effective.Often we persevere with various treatments, put the horse through much unnecessary suffering only to achieve an unsatisfactory outcome.
It is unlikely that there will ever be a single drug or other line of therapy to treat acute or chronic laminitis so our research efforts need to be directed toward prevention.
References
O'Grady, S.E. Realignment of P3 –the basis for treating chronic laminitis. Equine Vet Edu 2006; 8: 272-276.
Steward, M.L. How to Construct and Apply Atraumatic Therapeutic Shoes to Treat Acute or Chronic Laminitis in the Horse. in Proceedings. Amer. Assoc of Equine Pract 2003;49: 337-346..
Redden, R.F. Clinical and Radiographic Examination of the Equine Foot. in Proceedings. Am Assoc of Equine Pract 2003;49: 174-185.
Parks, A.H. Chronic Laminitis. In: Robinson NE, ed. Current Therapy in Equine Medicine. vol 5. St. Louis: W. B.Saunders, 2003:520-528.
Parks, A.H., O'Grady, S. E. Chronic laminitis: current treatment strategies.In: O'Grady SE, ed. The Veterinary Clinics of North America, vol. 19:2.Philadelphia: W. B. Saunders, 2003; 393-416.
Moyer, W., Schumacher, Jim,Schumacher, John. Chronic Laminitis:Considerations for the Owner and Prevention of Misunderstandings. in Proceedings. Amer. Assoc of Equine Pract 2000;46: 59-61.