Treating Chronic Laminitis - A Novel Approach Stephen E O'Grady, BVSc, MRCVS
Take home message
Chronic laminitis involves the distal displacement of P3, resulting in a shift of the weight- bearing function of P3 from its solar surface to the apex. The chronic pain and decreased sole growth which result, can only be ameliorated through realignment of P3; a process that historically has been difficult to achieve. In a small group of horses, a glue-on shoe technique has consistently corrected the alignment of P3 and has shown great promise as a treatment for chronic laminitis.
Introduction Chronic laminitis continues to be one of the most frustrating medical conditions facing veterinary practitioners, farriers and horseman. Laminitis can be defined as an idiopathic inflammation or ischemia of the submural structures of the foot.1 It can be further divided into developmental, acute, and chronic stages. If treatment during the acute stage of laminitis does not lead to full recovery, the disease will progress to the point where there is clinical and radiographic evidence of displacement of the distal phalanx (P3) within the hoof capsule.2 Stated another way, there is a failure of the attachment between the distal phalanx and the inner hoof wall. 2 The horse can now be considered to be in the chronic stage of laminitis. Clinical signs ranging from persistent mild to severe lameness, further mechanical collapse of the foot, recurrent abscesses, and hoof wall deformation, characterize the chronic stage. Because of the individualistic nature of chronic laminitis including the extent of damage to the lamellar tissue, the amount of rotation within the hoof capsule, individual foot conformation and hoof wall deformation, there has been no treatment that has been consistently successful for all cases. 3 Rehabilitation during the chronic stage attempts to reverse the mechanical changes that have occurred within the hoof by realigning the distal phalanx with its natural weight-bearing surface. Therapeutic trimming and shoeing has always been the "hallmark" of therapy in the chronic stage. Depending on the severity, it may be combined with a surgical release procedure such as an accessory ligament desmotomy or a deep digital flexor tenotomy. Present shoeing techniques seldom provide acceptable realignment of the distal phalanx. Over the past two years, a simple technique developed within the realm of glue-on technology has provided a method to realign the distal phalanx, which has given consistent beneficial results treating chronic laminitis.
Stages leading to chronic laminitis In the developmental stage of laminitis, the disease may originate in an area of the body far removed from the feet. The organ system involved may be the gastrointestinal, respiratory, reproductive, endocrine, immune or musculoskeletal. Aberrations in these organ systems can trigger a pathological process within the lamellar tissue of the foot. This process is triggered through a yet unexplained pathway. Rarely does the initiating cause of laminitis result in immediate clinical signs in the foot. The acute stage of the disease emerges with the onset of clinical foot pain.
Once clinical signs of laminitis are present, the clinical course of the disease is usually related to the quantity or severity of laminar damage that has occurred (Baxter G M, 1996) Along with foot pain, there is a bounding digital pulse; heat is present as well as one of the Obel grades of lameness. It is imperative to institute therapy during the developmental stage if possible or at the first sign of clinical foot pain, as the window of opportunity for medical treatment is extremely small.
Treatment regimens for acute laminitis remain empiric and are based on the past experience of the attending veterinarian. Treatment is directed towards eliminating or minimizing any predisposing factors, the judicious use of non-steroidal anti-inflammatory medications (NSAID), strict stall confinement and foot support that provides a biomechanical advantage. The chronic stage of laminitis
Chronic laminitis implies that mechanical or structural failure of the foot has occurred. 4 Mechanical failure is the displacement of the distal phalanx relative to the dorsal hoof wall. It can be described as rotation or vertical displacement (sinking). Rotation occurs when the dorsal parietal surface of the distal phalanx is distracted away from the dorsal hoof wall. Biomechanical forces that contribute to rotation are the vertical load of the horses weight on the digit and the forces exerted by the deep digital flexor tendon on the compromised lamina. 11 The amount of distal phalanx rotation depends on the load sustained by the foot and the number of compromised lamina. As the distal phalanx rotates, the dorsal coronary corium becomes compressed between the extensor process and the hoof wall leading to pressure-induced ischemia. 6 Rotation causes compression of the blood vessels and solar corium between the sole and distal phalanx. 1,6 This loss of circulation in the solar corium coupled with the pressure on the soft tissue inhibits sole growth, leads to further degeneration and causes persistent pain. This pain can be readily demonstrated in most cases by applying hoof testers to the sole in front of the frog. This continual pain may also play a role in the pain-hypertension cycle associated with laminitis by contributing to digital ischemia and requiring the continuous use of a NSAID.11-12 Rotation along with the unequal hoof growth seen with chronic laminitis tends to perpetuate pressure on the sole under the apex of the distal phalanx. Realignment is directed towards re-establishing the weight-bearing surface of the distal phalanx with the ground. When realignment of the distal phalanx is successful, the pressure is removed from the compressed tissue at the coronet and beneath the distal phalanx.
Different shoeing techniques have been described and any one may have merit in certain cases yet no single shoe or technique is suitable for all situations. 2 Corrective trimming of the hoof capsule attempts to realign the distal phalanx to its proper position in respect to the ground while maintaining an appropriate hoof pastern axis. 10 Trimming is often complimented by a certain type of shoe. Various factors such as stage and extent of the disease, individual foot conformation, protruding sole and limited available hoof wall, may prevent realignment through trimming alone. Radiographs
In the chronic stage of laminitis, radiographs are used to assess displacement of the distal phalanx within the hoof capsule and can be used for guidance when trimming the laminitic foot. A disciplined radiographic technique assures consistent, good quality films. The foot is placed on a positioning block, 3 x 5 x 7 inches, with a wire running through the long axis of the block. An opaque marker such as a wire is placed on the dorsal hoof wall and a thumbtack is placed near the apex of the frog. The opposing limb should be placed on a block of equal height. The primary beam should strike the foot in a horizontal plane, just above the ground surface so that it is centered on the solar margin of the distal phalanx. 5
 In the chronic stage, abnormalities observed on radiographs include the presence of capsular or phalangeal rotation, vertical distal displacement of the distal phalanx (sinking), sole depth present, laminar thickening and remodeling of P3. It may be helpful to distinguish between capsular rotation and phalangeal rotation. 1 Capsular rotation (Figure 1) describes divergence of the hoof capsule away from the dorsal parietal surface of the distal phalanx regardless of the angulation of the distal phalanx. Phalangeal rotation describes the distal phalanx in relation to the rest of the phalangeal axis regardless of capsule position. Understanding the different types of rotation may prove beneficial when re-alignment of the distal phalanx is attempted. In the chronic stage, abnormalities observed on radiographs include the presence of capsular or phalangeal rotation, vertical distal displacement of the distal phalanx (sinking), sole depth present, laminar thickening and remodeling of P3. It may be helpful to distinguish between capsular rotation and phalangeal rotation. 1 Capsular rotation (Figure 1) describes divergence of the hoof capsule away from the dorsal parietal surface of the distal phalanx regardless of the angulation of the distal phalanx. Phalangeal rotation describes the distal phalanx in relation to the rest of the phalangeal axis regardless of capsule position. Understanding the different types of rotation may prove beneficial when re-alignment of the distal phalanx is attempted.
Glue-on technology
Glue-on technology has been available since 1986. Historically, the techniques have employed the outer hoof wall by using a cuff or plastic tabs for attaching a shoe.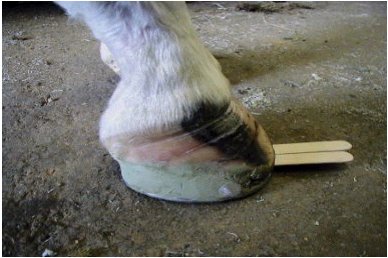 A method described recently uses the solar surface of the hoof with the shoe glued directly to the bottom of the foot. 9 A polymethylmethacrylatea (composite) combined with fiberglass strands are used to attach an aluminum shoe to the foot. In the case of the laminitic horse with rotation, using radiographic guidance, the palmar surface of the foot can be used to realign the distal phalanx in order to create a more parallel relationship with the ground. This is accomplished through trimming and by varying the amount of composite / fiberglass used to attach the shoe to the foot thereby changing the angle of the shoe relative to the foot. Realignment of the distal phalanx will lift the toe off the shoe causing weight bearing to be localized palmarly and it removes pressure placed on the lamina and solar corium in the toe area (figure 3). A method described recently uses the solar surface of the hoof with the shoe glued directly to the bottom of the foot. 9 A polymethylmethacrylatea (composite) combined with fiberglass strands are used to attach an aluminum shoe to the foot. In the case of the laminitic horse with rotation, using radiographic guidance, the palmar surface of the foot can be used to realign the distal phalanx in order to create a more parallel relationship with the ground. This is accomplished through trimming and by varying the amount of composite / fiberglass used to attach the shoe to the foot thereby changing the angle of the shoe relative to the foot. Realignment of the distal phalanx will lift the toe off the shoe causing weight bearing to be localized palmarly and it removes pressure placed on the lamina and solar corium in the toe area (figure 3).
Method
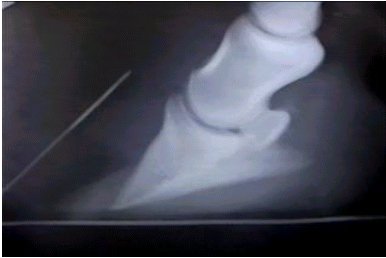
To realign the foot, a line is drawn on the radiograph through the removable portion of heel and continuing the length of P3 while staying parallel to the solar surface of P3. The distance from P3 to the line drawn from the heels forward should remain constant throughout the length of the third phalanx. Another line is drawn below the first to simulate the shoe. If you take the radiograph and turn the film so the lines on the solar surface are in a horizontal plane-this will show an acceptable alignment of the distal phalanx with the ground. (figures 4,5,6,7) The distance between the shoe and the foot that will be necessary to achieve this alignment can be measured from the radiograph. The point where the shoe should breakover can also be determined from the radiograph using the opaque marker that was placed in the frog. The distance is measured from the opaque marker to the apex of the distal phalanx and marked on the foot.  Fig. 4 Fig. 4 | 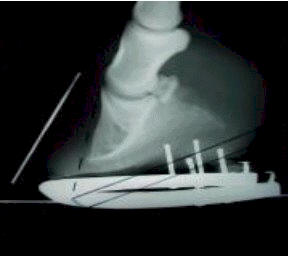 Fig. 5 Fig. 5 | 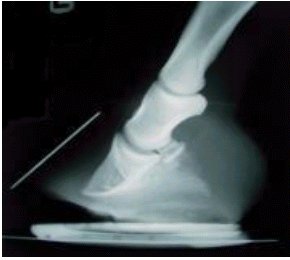 Fig. 6 Fig. 6 |  Fig. 7 Fig. 7 |
The heels are lowered with a rasp starting at a point just behind the apex of the frog. It is prudent to reach solid hoof wall at the heels if possible. A St Croix aluminum shoe is fitted to the foot being sure that the branches of the shoe extend beyond the heels of the foot. This extra length will increase solar surface area, move weight bearing palmarly and decrease tension in the deep digital flexor tendon. The trimmed part of the foot is rinsed with denatured alcohol. Two 4-inch by 4-inch square of fiberglass mesh are pulled apart to separate the strands. 2-3 ounces of the composite is then mixed with each pile of fiberglass. This combination gives the composite bulk, makes it easier to mold and adds structural strength. Using gloves, a thin layer of the plain composite is applied to the area of the hoof to be bonded, working it into the surface. This will improve the contact area to be bonded. The combined composite and fiberglass is then picked up and molded (rolled) into a tubular structure. One roll is placed on either side of the prepared foot starting at the apex of the frog and extending beyond the heel (Figure 8). The fitted shoe is then placed on the hoof and pressed into the composite to the predetermined position so that the angle of the shoe is such that the shoe parallels the solar surface of P3. It is easy to adjust the shoe angle in any direction by just molding the tubular structure of the composite thicker or thinner to achieve the desired effect. The foot is held off the ground until the composite sets, which is usually two or three minutes depending on the ambient temperature. Placing an elastic polymer on the frog and sole, which helps to evenly distribute the weight bearing, can provide additional support. B Using gloves, a thin layer of the plain composite is applied to the area of the hoof to be bonded, working it into the surface. This will improve the contact area to be bonded. The combined composite and fiberglass is then picked up and molded (rolled) into a tubular structure. One roll is placed on either side of the prepared foot starting at the apex of the frog and extending beyond the heel (Figure 8). The fitted shoe is then placed on the hoof and pressed into the composite to the predetermined position so that the angle of the shoe is such that the shoe parallels the solar surface of P3. It is easy to adjust the shoe angle in any direction by just molding the tubular structure of the composite thicker or thinner to achieve the desired effect. The foot is held off the ground until the composite sets, which is usually two or three minutes depending on the ambient temperature. Placing an elastic polymer on the frog and sole, which helps to evenly distribute the weight bearing, can provide additional support. B
Results
During the last twelve months, eighteen horses with chronic laminitis have been treated with glue-on shoes using the described method. All horses had the disease greater than three months, all had greater than ten degrees of rotation, all were painful to hoof testers and all had at least Obel grade 2 (1-4) lameness. All eighteen horses had shoes glued on using radiographic guidance to realign the solar surface of the distal phalanx so that it parallels the ground surface. Combined with the shoeing, three horses had a deep digital flexor tenotomy and one horse had an inferior check ligament desmotomy.
Following the procedure all horses were confined to the stall for three weeks followed by two weeks of brief hand walking once daily. The shoes were reset in five weeks.
At the first reset, hoof tester pain was decreased, there was 3 to 5 mm of new sole growth, increased hoof wall growth was noted below the coronet at the toe and all had decreased at least one Obel grade of lameness.
At the third reset, hoof wall and sole growth both improved to the extent where progressive realignment could be continued using the hoof capsule. Shoes were attached in a conventional manner using nails. Although not all horses were sound, the lameness was improved in all cases to where controlled turn out could be initiated.
Surgical treatment
If the foot deformity is such that the distal phalanx cannot be successively realigned with trimming and shoeing, then surgical intervention is indicated. Inferior check ligament desmotomy and deep digital flexor tenotomy are the two surgical procedures used to treat chronic laminitis. 7,8; 10-12 It is often hard to select which cases should have surgery, when the surgery should be done and which surgery should be performed. 11 The rationale for performing either surgery is to release the distraction of the deep digital flexor tendon on the distal phalanx. Either procedure will provide tendon release, which permits alignment of the P3 with the ground and correction of the hoof deformity. The amount of tension release with inferior check ligament demotomy compared to deep digital flexor tenotomy is much less. Which surgery to perform can be based in part on duration, mobility of the animal, level of pain, recurrent sepsis, hoof wall deformation and hoof pastern axis. If a significant flexure deformity of the distal interphalangeal joint is present radiographically, then some form of tendon release procedure is indicated. 10
To be most effective, the inferior check ligament desmotomy or the tenotomy should be combined with therapeutic shoeing designed to realign the weight-bearing surface of the distal phalanx with the ground. 7,8,12 We elect to do the therapeutic shoeing before the surgical procedure is performed.
Discussion
It is our contention that if possible, the chronic laminitic horse should not be shod until it is comfortable with minimal medication along with clinical and radiographic indications that the foot has stabilized. The laminar damage may be so extensive in many cases that recovery will not be possible or it may preclude rehabilitation of the feet during the chronic stage. There has been a multitude of farrier techniques proposed to treat chronic laminitis, some have been helpful, many have been of little value and none have been consistent. 2,15 In normal horses, the angle made by the distal solar border of the distal phalanx with the ground is reported to be anywhere between 2-10 degrees, though the average is probably between 3-6 degrees. 13,14 If one looks at the mechanics of rotation, this angle increases as the distal phalanx rotates distad. Significant rotation results in weight bearing being concentrated on the apex of the distal phalanx along with compression of the dermal tissue located at the dorsal coronet and beneath the third phalanx. In order to reverse these changes within the hoof capsule, treatment should be directed toward realignment of P3. With capsular rotation or mild phalangeal rotation, there is generally insufficient hoof wall present in the heel area that can be trimmed to achieve realignment of P3. Even when the heels are lowered significantly, it generally does not allow the distal phalanx to assume a normal position relative to the ground nor does it remove pressure from the toe. Glue-on technology provides a relatively simple method to realign P3 in the chronic laminitic horse. Using radiographic guidance the breakover is moved back thus reducing the opposing lever arm. Next, the proper angle of the shoe is determined such that the shoe parallels the solar surface of P3. A polymethymethcrylate is used to attach the shoe at this angle, thus realigning P3 with the ground. In so doing, weight bearing is restored to the solar surface of P3, compression of the solar corium is relieved, pain ameliorated and sole growth promoted. Additionally, glue-on shoes provide a way to shoe a chronic laminitic horse in a non-traumatic manner.
References
1. Hood DM. Laminitis in the horse. Vet Clin North Am Equine Practice 1999;15:287-293, 437-463.
2. Pollitt CC. Equine laminitis: a revised pathophysiology. in Proceedings. 45th Annu Conv Am Assoc Equine Practnr 1999;189-192. 3. Moyer W, et al. Chronic laminitis: Considerations for the owner and prevention of misunderstandings, in Proceedings 46th Annu Conv Am Assoc Equine Practnr 2000;59-61. 4. Hood DM. Treatment of chronic laminitis. in Proceedings Dodson and Horrell International Conference on Laminitis 1998;7-15. 5. Redden RF. Shoeing the laminitic horse. in Proceedings 43rd Annu Conv Am Assoc Equine Practnr 1997;356-359. 6. Goetz TE. Anatomic, hoof, and shoeing considerations for the treatment of laminitis in horses. J Am Vet Med Assoc 1987;190:10, 1323. 7. Eastman TG, et al. Deep digital flexor tenotomy as a treatment of chronic laminitis in horses: 35 cases (1988-1997) J Am Vet Med Assoc 1999;214:517-519 8. Turner TA, O'Grady SE, Tempeleton RS. Use of deep digital flexor tenotomy in the management of laminitis. In Proceedings 38th Annu Conv Am Assoc Equine Practnr 1992;11-12. 9. O'Grady SE, Watson E. How to glue on therapeutic shoes. In Proceedings 45th Annu Conv Am Assn Eq Practnr 1999;115-119. 10. White NA. Treatment and shoeing for the laminitic horse. in Proceedings 10th Annual ACVS Symposium. 2000;294-298 11. Hunt RJ. Diagnosing and treating chronic laminitis Vet Med 1996; 91:11,1025-1032. 12. O'Grady SE. A practical approach to treating laminitis. Vet Med 1993;88:9, 867-875. 13. Cripps PJ, Eustace RA. Radiological measurements from the feet of normal horses with relevance to laminitis. Equine Vet J 1999;31:5, 427-432. 14. Linford RL, O'Brien TR, et al. Qualitative and morphometric radiographic findings in the distal phalanx and soft tissues of sound thoroughbred racehorses. Am J Vet Res, 1993;54:1, 38-51. 15. Moyer W, Redden RF: Chronic and severe laminitis: a critique of therapy with heart bar shoes. Equine Vet J 1989;21:5, 317-318. Footnotes:
a. Equilox? - Equilox Int'l 110 NE 2nd Street, Pine Island, MN 55963
b. Advance Cushion Support ---Advance Equine P.O. Box 54 Versailles, KY 40383 |