"Reprinted with permission from the Journal of Equine Veterinary Education.
Original article appeared in Equine Veterinary Education American Edition April 2001 "
| Introduction Keratoma is an uncommon tumor of the keratin producing epidermal cells of the inner hoof wall (Lloyd et al 1988). It is rare to find a keratoma located in the dermis of the sole and there is little information reported in the literature regarding occurrence in this region. Keratomas result from proliferation of cornified tissue on the inner side of the hoof wall (Chaffin et al 1989). They are interposed between the stratum medium of the hoof wall and underlying third phalanx and can be located any where from the coronet to the solar surface of the foot at the white line. They can be cylindrical or spherical in shape and are generally found in the toe or the quarters of the hoof. Keratomas are slow- growing tumors and its not until the increasing size exerts pressure on the laminar dermis and the surface of the third phalanx that lameness becomes apparent (Honnas et al 1988). Aetiology remains obscure, but it is thought to result from trauma or chronic irritation from direct hoof injury or sole abscesses (Honnas et al 1994). This report describes a keratoma found in the dermis of the sole leading to an elusive lameness. History A 12-year-old Warmblood gelding was presented for consultation with a history of having persistent right hindlimb lameness. The lameness (Grade 2 to Grade 4 of Grades 1-5) had an insidious onset and had been present for the previous two months. Focal discomfort was evident when hoof testers were applied over the sole of the lateral quarter. At the initial examination, haemorrhage was noted when the sole was superficially pared away over the painful area. An initial diagnosis of a foot abscess or subsolar bruising was made and the horse was treated with hot soaks, poultice and anti-inflammatory medications. As the lameness persisted, periodic radiographs where taken, but no abnormalities were identified. The lameness was abolished by lateral posterior digital nerve block and by intra-articular anesthesia of the distal interphalangeal joint. Various shoeing methods were used, including a shoe with a rim pad, to remove any pressure on the sole. Interestingly, lameness increased when the horse was shod and improved when allowed to remain unshod. Physical Examination When examined, the horse was unshod and walking well. Surgery
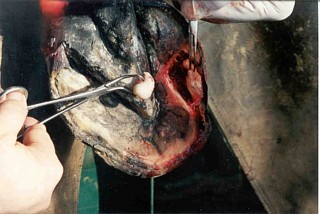 Fig. 4
Aftercare The horse was treated with sulfamethoxazole/Trimethoprim (30 mg/kg bwt per os b.i.d.) for five days following surgery. Histopathology The 2 x 1.5 x 1 cm. teardrop-shaped mass was submitted for histopathology. The tumor was composed of lamellated keratin. On cross section it had an "onion skinned appearance and was covered with a thin layer of flattened orderly squamous epithelium. Diagnosis was a keratoma. Discussion The initial presentation, foot-related lameness, associated with a focal area of pain, with the lameness abolished by anesthesia of the palmar digital nerves, is a common presentation in equine practice. Usual differential diagnosis for this presentation should include subsolar abscess or bruising, puncture wound, focal osteomyelitis and a marginal fracture of the third phalanx. However, in this case there was no tract or puncture found in the sole or white line nor was there discoloration on the outer surface of the sole. In addition, consecutive radiographs failed to reveal a fracture. The diagnosis of a solar keratoma is uncommon. Although palmar digital anesthesia confirmed the foot as the source of pain, the block was not specific for the problem. It is unlikely that anesthesia of the distal interphalangeal joint would have provided additional information, as recent studies have shown that local anesthesia injected in the DIP joint will block the dermis of the anterior portion of the sole (Schumacher et al. 1999). Indications that a mass might be present were that when a shoe was applied the lameness increased from Grade 2 to Grade 3 or more. Additionally, the lameness subsided when the shoe was removed. This suggested that when the horse bore weight, impingement of a mass interposed between the shoe and the inner structures of the foot resulted in pain. An insidious onset of lameness is often the presenting complaint with keratoma (Honnas 1998). Over time, diagnostic indications of a solar mass become more obvious. In long standing cases of keratoma of the hoof wall, focal thickening or inward deviation of the white line becomes apparent. If a tumor enlarges over time, it causes increasing pressure on the third phalanx leading to a focal area of bone resorption (Lloyd et al. 1998). Pressure is also placed on the overlying epidermis of the sole causing it to become convex (bulge). This pressure also leads to thinning and discoloration of the overlying sole. In conclusion, unresolved lameness with pain localized to a focal area of the sole can present a diagnostic challenge. With persistent lameness localized to a small section of the sole, keratoma within the dermis of the sole or other tumors of the equine hoof should form part of the differential diagnosis. 1 Castle Plastics, Leominster, MA 01453 2 Essex Tierarznei, Munich, Germany References Chaffin MK, Carter GK. Sustaire D. (1989) Management of a Kurimoto in a horse: A case report. Equine vet Sci. 9,323. Honnas, C.M. (1998) Keratomas of the equine digit. Equine vet Educ. Manual 4, 68-72. Honnas CM, Meagher DM, Linford RL: (1988) Surgical management of difficult foot problems in the horse: current concepts. Proc Am Assoc Equine Pract 34,249. Honnas CM, Pelsos JG, Carter GK, Moyer W. (1994) Surgical management of incomplete avulsion of the coronary band and keratomas in horses. Vet Med 89, 984-988. Lloyd KCK, Peterson PR, Wheat JD, Ryan AE, and Clark JH. (1988) Keratomas in horses: Seven Cases (1975-1986). J Am Vet Med Assoc 193, 967-970. Schumacher, J., Schramme, M., Schumacher, Jim, DeGraves, F., Steiger, R., and Coker, M. (1999) Abolition of lameness caused by experimently induced solar pain in horses after analgesia of the distal interphalangeal joint. Proc. Am. Ass. Equine Practnrs. 45, 193-194. |
 Grade 2 lameness was observed when the animal was trotted on a hard surface. The conformation of the foot was normal with respect to size, shape and angle. There was a focal, discolored (haemorrhagic), slightly convex section of sole medial to the white line in the lateral quarter of the hoof. The architecture of the white line in this area was not distorted nor were there any separations or tracts. Again, pain was elicited to hoof testers but the area was also sensitive to digital pressure. At this juncture, examination of further radiographs showed a small convex area of osteolysis or bone resorption on the plantar surface of the third phalanx on the lateral view (Fig 1). The dorso-ventral view of the third phalanx was unremarkable. Because these findings were indicative of a mass causing the lysis of the third phalanx, it was decided to surgically explore this section of the foot.
Grade 2 lameness was observed when the animal was trotted on a hard surface. The conformation of the foot was normal with respect to size, shape and angle. There was a focal, discolored (haemorrhagic), slightly convex section of sole medial to the white line in the lateral quarter of the hoof. The architecture of the white line in this area was not distorted nor were there any separations or tracts. Again, pain was elicited to hoof testers but the area was also sensitive to digital pressure. At this juncture, examination of further radiographs showed a small convex area of osteolysis or bone resorption on the plantar surface of the third phalanx on the lateral view (Fig 1). The dorso-ventral view of the third phalanx was unremarkable. Because these findings were indicative of a mass causing the lysis of the third phalanx, it was decided to surgically explore this section of the foot. The procedure was done standing with the horse sedated using xylazine (1.1 mg/kg, IV) and butorphanol (0.1 mg/kg, IV). The foot was desensitized with a biaxial plantar nerve block just proximal to the sesamoid bones. An Esmarch's bandage was applied to the lower limb to control hemorrhage and aid visualization during surgery. The hoof was prepared aseptically with povodine iodine and alcohol. A thin looped hoof knife (Fig 2) was used to cut a trough around the perimeter of the lesion (Fig 3). The dissection was continued through the sole until a cavity was entered. The overlying flap of cornfield sole was laid back and a mass removed (Fig 4). The cavity was curretted down to normal healthy bone and the overlying flap of epidermis was removed. Silver sulphadiazine ointment was placed in the wound and the cavity loosely packed with gauze. An impervious bandage was placed on the foot.
The procedure was done standing with the horse sedated using xylazine (1.1 mg/kg, IV) and butorphanol (0.1 mg/kg, IV). The foot was desensitized with a biaxial plantar nerve block just proximal to the sesamoid bones. An Esmarch's bandage was applied to the lower limb to control hemorrhage and aid visualization during surgery. The hoof was prepared aseptically with povodine iodine and alcohol. A thin looped hoof knife (Fig 2) was used to cut a trough around the perimeter of the lesion (Fig 3). The dissection was continued through the sole until a cavity was entered. The overlying flap of cornfield sole was laid back and a mass removed (Fig 4). The cavity was curretted down to normal healthy bone and the overlying flap of epidermis was removed. Silver sulphadiazine ointment was placed in the wound and the cavity loosely packed with gauze. An impervious bandage was placed on the foot.
 Phenylbutazone (4.4 mg/kg bwt per os) was used only as needed for pain relief. The bandage was changed at 4-day intervals and the wound was packed with silvadine ointment. Granulation tissue filled the cavity rapidly and was level with the surrounding sole at the third bandage change, at which time a bar shoe with a treatment plate, that had been constructed and fitted prior to the surgery, was applied to the foot. The treatment plate was made from high-density plastic 1 which is light and resists wear (Fig 5). At this point the topical medication was changed to Lotagen Gel 2 to increase toughness of keratinised epithelium and the dressing was changed every other day. Forty-five days post surgery; the horse was sound and started in light exercise.
Phenylbutazone (4.4 mg/kg bwt per os) was used only as needed for pain relief. The bandage was changed at 4-day intervals and the wound was packed with silvadine ointment. Granulation tissue filled the cavity rapidly and was level with the surrounding sole at the third bandage change, at which time a bar shoe with a treatment plate, that had been constructed and fitted prior to the surgery, was applied to the foot. The treatment plate was made from high-density plastic 1 which is light and resists wear (Fig 5). At this point the topical medication was changed to Lotagen Gel 2 to increase toughness of keratinised epithelium and the dressing was changed every other day. Forty-five days post surgery; the horse was sound and started in light exercise.