An Overview Of Equine CankerReprinted with permission from the American Farriers Journal. |
|
|
Clinical Signs Of Canker
Canker generally originates in the frog and can be mistaken for thrush in the early stages. Thrush is limited to the frog and results in a very recognizable deterioration or loss of frog tissue where on the other hand there is a proliferation of tissue with canker (Figure 1).
Canker may present anywhere from a focal area of granulation tissue in the frog that bleeds easily when abraded to long filamentous fronds of hypertrophic horn.Canker is characterized by numerous small finger-like papillae consisting of a soft,off-white material that resembles a “cauliflower-like’ appearance and is covered with a caseous white exudate that resembles cottage cheese (Figures 2 and 3a-3c).
 |
| Figures 3A, 3B & 3C: Figure 3A (left) shows filamentous fronds of hypertrophic horn. Figure 3B (center) shows the finger like papillae that presents a “cauliflower” appearance. Figure 3C (right) shows a white caseous exudate that resembles “cottage cheese” beneath the outer hard layer of the frog. The condition is frequently, but not always, accompanied by a foul odor. |
The condition is frequently, but not always, accompanied by a foul odor.However, if any type of antiseptic or caustic medication has been used for treatment, the smell will disappear. The affected tissue will bleed easily when abraded and maybe extremely painful to the horse when touched or pressure is applied. Varying degrees of lameness will be present depending on the extent and depth of the infection. Most horses are not lame if the disease is recognized and treated early.
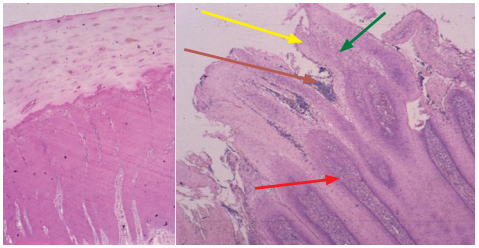 |
| Figure 4: Photomicrograph on the left shows normal epidermis/dermis of frog. Photomicrograph on the right shows the tissue affected with canker.Red arrow is papillary hyperplasia, green arrow is keratolysis, yellow arrow is degeneration of the outer layer of the epidermis and blue arrow is a mixed population of bacterial organisms. |
Diagnosis Of Canker
A presumptive diagnosis of canker is based on ruling out the presence of thrush,the gross appearance of the affected horny tissue covering the frog, a fetid odor and the ease with which the abraded tissue bleeds. However, a definitive diagnosis may be confirmed with a biopsy. Biopsy is most useful in recurrent cases or when the lesions do not have the characteristic appearance or location in the foot.
Histologically, the lesion is read as a“chronic hypertrophic moist pododermatitis.” It is characterized by a proliferative papillary hyperplasia of the epidermis with dyskeratosis, keratolysis and ballooning degeneration of the outer layers of the epidermis. A mixed population of bacterial organisms are observed in the stratum germinativum layer of the epidermis of the frog (Figure 4). Cultures per se are unrewarding as they typically produce an assortment of environmental organisms such as “Bacteroides sp.” and“Fusobacterium necrophorum,” the usual opportunistic bacteria found in the solar surface of the horse’s foot.
 |
| Figure 5: No canker present in the frog, but note how the foot should be prepared prior to debridement. Note the slope of the bars for exposure of frog sulci. |
Treatment Of Canker
Treatment of canker is a realistic example of a joint venture between a veterinarian and a farrier. From a legal and ethical standpoint, working with dermal tissue is the practice of veterinary medicine. The effective veterinary treatment of canker requires sedation, local anesthesia,surgery (debridement without hemorrhage)and medication. Many veterinarians are not familiar with farrier tools or their use,unable to trim and prepare the foot prior to debridement, are unable to explore the hoof capsule appropriately and are unable to provide the necessary follow-up farriery care. This describes the farrier’s role and input. Treatment should be considered a team approach with the veterinarian, farrier and owner/caregiver
Trimming and preparation of foot. An important aspect that is often overlooked is to trim the foot prior to surgery. Try to address any hoof capsule distortion at the onset in order to give the foot a mechanical advantage. All loose exfoliating sole is removed from the solar surface of the foot. The bars and sole of the hoof capsule adjacent to the frog are explored to be sure the horn in this area is not involved. All underrun or loose horn is removed down to solid structures (Figure 5).
 |
| Figure 6: Esmark bandage in place. |
The heels are trimmed such that the hoof wall at the heels and the frog are on the same plane or approach the same plane.The frog should not be recessed between the heels of the hoof wall at the beginning of treatment or the affected tissue will not heal. I also trim the bars on more of a slope than usual because I want good exposure to the sulci around the frog. After the foot is prepared with the appropriate farriery,soaking the foot with any of the various cleaning solutions or products is unnecessary. The foot is now placed in a bucket of clean water and the foot is scrubbed thoroughly with an antiseptic soap using a firm brush. I prefer to do the debridement standing under local anesthesia but it can be done under general anesthesia if there are behavior issues with the horse or at the discretion of the clinician.
Debridement. A tourniquet such as an Esmark bandage or a length of tire inner tube cut at a 3-inch width is placed starting at mid-pastern to above the fetlock (Figure 6). It is essential to create a bloodless field so the demarcation between normal and diseased tissue can be seen during debridement. All abnormal tissue is removed until the tissue resembles a pink velvet color with numerous pin-point hemorrhages, which are the dermal papilla (Figure 7).
Remember that canker is generally limited to the epidermis, so debridement needs to be careful, gentle, thorough and wide rather than aggressive, deep and radical, which often leads to unnecessary removal of the dermal tissue under the lesion. This tissue is necessary for re-growth of healthy horn and cornification. For debridement, I use a small pair of rongeurs to remove the bulk of diseased tissue, a sharp loop knife and a #12 scalpel blade (Figure 8).
|
|
After the bulk of the diseased tissue is removed, the remaining layers of diseased tissue just peel off in strips with the loop knife and the blade is used in the tighter more obscure areas. The debridement is followed by cryotherapy to freeze the area that has been debrided to remove residual bacteria from the surface in a double freeze-thaw, freeze-thaw pattern using a commercially available coolant spray.
Aftercare Of Canker
There are a variety of topical preparations that can be used following debridement but the astringents (drying agents) may play the most important role.I use 4-inch x 4-inch gauze sponges moistened in a solution of 10% benzoyl peroxidein acetone, sprinkled with metronidazole powder placed over the debrided site. There are other topical products available such as dry dressings that have been soaked in a solution of tricide/gentocin/lincomycin and an oxytetracycline/metronidazole paste that may be equally effective. No caustic preparations should ever be used as they will burn or damage the dermal tissue trying to restore healthy horn.
The foot is then bandaged using any combination of products — baby diapers attached with a cohesive bandage is a very inexpensive option. A shoe with a treatment plate has become popular with canker cases, but I feel it is contraindicated as it neither keeps the foot as clean or as dry as necessary post debridement. Once the surface has a complete layer of thin cornification, a treatment plate can be used if desired.
Client compliance. Owner compliance for the aftercare is critical for a successful outcome. The bandage is changed daily for the first 7 to 10 days, and then at least every second day. At each bandage change,the affected area is cleaned gently with an antiseptic solution (not antiseptic soap),rinsed with free-flowing saline and dried with a paper towel. The topical medication of choice is applied and the foot is rebandaged. It is crucial to keep the animal in a dry environment such as a small dry lot or a stall bedded in saw dust or wood shavings
The owner should look for any focal or small reoccurrences of disease in the debrided surface at each bandage change. If an area of abnormal growth is noted, these are managed with light debridement using a dry gauze sponge followed by cryotherapy.The foot should be fully cornified within 3 to 6 weeks and a treatment plate can be applied at that time if desired (Figure 9).
 |
| Figure 9: Before and after pictures of a canker case. After picture is 2 weeks post debridement. |
Corticosteroids. There appears to be an immune-mediated component to canker as the corticosteroids make a profound difference in the outcome of the case. I put all cases on a descending dose of oral prednisolone during the treatment phase of canker(generally 4 weeks).3,4
Discussion
I reported with Florida veterinarian John Madison on 60 horses with canker in 2004 and then published an update on equine canker with North Carolina State University vet Rich Redding in Veterinary Clinics of North America —Equine Practice in 2012.I now have over 150 horses in the database.The treatment of equine canker has always presented a dilemma for veterinarians and farriers due to the historically poor prognosis. The etiology of canker remains obscure. However, the disease can be consistently and effectively treated. It does not appear to be a disease of horses caused by poor care or unhygienic conditions. In the database, most of the horses treated were well cared for and received routine hoof care. While the hind limbs seemed to be affected more frequently, forelimb involvement is common.
Trimming the foot, thorough debridement and owner commitment are important for a successful outcome of this condition. Careful and thorough wide debridement of the lesion is essential, rather than aggressive radical debridement with the common connotation“cut it all out.” The dermis has to be spared in order for healthy epidermis to be produced and cornified. Emphasis must be placed on keeping the surgical wound clean and dry until the defect has completely cornified.Owner compliance to perform the daily footcare is always a critical and essential element in the treatment of equine canker.
REFERENCES



