| How to Treat Coronary Band Dystrophy Stephen E. O’Grady, DVM, MRCVS Reprinted with permission from the American Association of Equine Practitioners. Introduction Coronary band dystrophy (CBD) appears to be increasingly recognized and diagnosed in equine veterinary practice as a distinct dermatological disease that affects the equine coronet. However, the information on this disease in the equine veterinary literature is sparse.1–4 The disease is frustrating to treat, labor intensive on the part of the caregiver, and is often non-responsive to treatment. CBD is described as an idiopathic defect in cornification of the coronary band that predominately affects the heavy breeds of horses,a,b but in the study described in this paper, the cases were either Warmblood or Warmblood-cross horses. There appears to be no apparent age or gender predisposition, all four hooves are generally affected to a variable extent, and long-term treatment may often be palliative rather than curative.1 An immune-mediated pathway appears to be the logical explanation as the disease is responsive to systemic corticosteroids and recently, a report describing methotrexate being used to treat CBD appears to be promising.c The response to these two drugs may indicate that the term, CBD, is not actually correct and that chronic immune-mediated coronitis may be more appropriate. A form of pemphigus foliaceus termed pemphigus coronitis has been incriminated but has not been completely proven. This report describes the successful (although it must be emphasized, not curative) treatment of greater than 20 horses that were diagnosed with CBD. Interestingly, 7 horses subsequently developed chronic proliferative pododermatitis (canker) secondary to CBD. Materials and Methods The records of 18 horses treated for CBD from 2015 until the end of 2019 were reviewed. Horses were selected from referral cases that had severe clinical signs of hyperkeratosis of the coronary bands involving all 4 feet and where other causes for these lesions could be excluded. The form of hyperkeratosis noted consisted of the formation of thick crusts on the coronet, showed hemorrhage and ulceration when removed, interfered with normal hoof wall growth, and did not respond to routine veterinary care. Furthermore, the lesions were not limited to the coronet but also appeared on the bulbs of the heels and the base of the frog. The breed distinction was either Warmblood or Warmblood crossed with Thoroughbred. Interestingly, quite a few of these horses (6) were imported to the United States at least a year prior to showing clinical signs. Sex was divided into 10 geldings, 7 mares, and 1 stallion and were aged between 7 and 18 years. The bulk of the cases were either treated by or personally overseen by the author while the remainder of the horses were treated through the author’s consulting practice and although there were good follow-up reports from the caregivers, the results could not be personally verified.
Clinical Signs When the horse is presented with CBD, the horse may or may not show lameness depending on the extent of the disease. In general, the coronary bands are proliferative with crusting, scaling, variable erythema, and often ulceration. In some instances, the ergots and chestnuts are also affected with the same lesions.1–4 Hooves may be thickened with poor consistency of the hoof wall, irregular ridges, scaling and closely packed growth rings. While the severity of the disease may vary, the initial changes at the coronary band may be subtle but can rapidly progress until the clinical signs are apparent. Generally, the hair that lays flat against the proximal coronet will begin to rise off the coronet and the proximal extent of the coronet will begin to thicken. As the disease progresses, a thin bead of dark brown, eroded, soft horn will be noted just below the hair and the hair will begin to stick straight out. At this point, hoof wall growth distal to the coronet will decrease as noted by the tightly packed growth rings (Fig. 1). Over time, the coronet at the hairline will swell, the bead of soft horn will enlarge, and the hoof wall below the abnormal horn will show crusts and scaling. The abnormal horn will start to widen toward the heels and then extend over the bulbs of the heels down to the frog (Fig. 2, A and B).
In the palmar or plantar section of the foot, the abnormal growth at the coronet at the heels will grow down into the hoof capsule and the crusted horn will grow distally and cover the bulb extending to the frog. The hair overlying the bulbs will now be standing erect. The crusted horn will often crack, ulcerate, and a clear serous exudate may be present. At this point, the abnormal horn may extend onto the surface of the frog if the frog is located below the ground surface of the hoof wall at the heels or ultimately may develop canker if the frog is recessed between the walls of the hoof capsule. In some cases, the thick crusted horn that covers the bulbs of the heels and the base of the frog will turn into a light brown, soft epithelium that is covering a caseous white exudate that resembles cottage cheese. This type of tissue is indicative of proliferative pododermatitis or canker.5 Horses may be lame if the CBD is so severe that there is ulceration at the coronet, a deep fissure present at the base of the diseased frog or the horse has developed canker (Fig. 3). A complete blood count and serum chemistry was performed on each horse and found to be within normal limits.
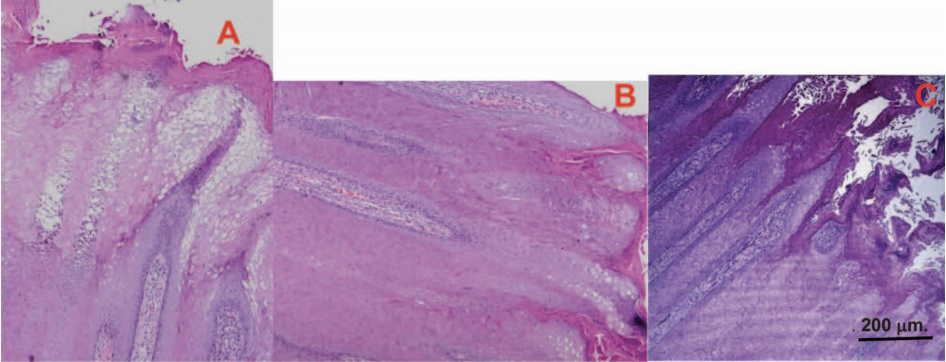
Diagnosis A tentative diagnosis is made on the clinical appearance and progression of the lesions localized to the coronet and heel bulbs. A definitive diagnosis is attained by ruling out other skin lesions such as pemphigus foliaceus, eosinophilic exfoliative dermatitis, dermatophilosis, zinc deficiency, selenium toxicity and infestation with Chorioptes equi. 1,3 The diagnosis can be confirmed with a biopsy. It should be noted that confirmation of pemphigus requires immunofluorescence staining which is not commonly done nor commonly available.d An incisional biopsy was obtained under local anesthesia from the coronet at the junction of the heel quarter and the heel bulb. The biopsy reports in this study showed the epidermis to be hyperplastic with marked acanthosis and the formation of long papillary fronds in the dermis. A moderate layer of orthokeratosis hyperkeratosis covered the surface of the epithelium over the coronary band dermis (Fig. 4A). Increased numbers of lymphocytes and plasma cells can be seen in the dermal papilla (Fig. 4B). The presence of lymphoid cells in the dermis is potentially compatible with an immunemediated condition.c A recently published pathology paper has an excellent photomicrograph of a section of the coronet illustrating the histology of CBD (Fig. 4C). As the biopsies were similar in the first few cases in this report, biopsies were discontinued because the wounds were difficult to heal.
Treatment Medication Treatment is labor-intensive and an owner/client commitment is necessary for success. The horse is placed on a descending dose of oral prednisolone administered at 1 mg/kg q24h for 10 days, 0.5 mg/ kg, q24h for 10 days, and 0.25 mg/kg, q24h for 10 days.6 After 30 days, the dose is continually decreased, and the days of administration are spaced further apart until the lowest possible dose to prevent reoccurrence is administered once or twice weekly. Also, at the onset of treatment, minocyclinef is given orally at 4 mg/kg, q12h in an attempt to treat any possible low-grade infection present in the coronary band.7 Firocoxibg is given orally at 171 mg, q24h for 3 days as a loading dose,8 and the 57 mg, q24h for a total of 14 days. This anti-inflammatory medication is used to counteract inflammation and discomfort associated with the initial debridement and subsequent daily debridements. Topical Treatment of the Coronet If the clinician does not perform this type of work, the initial foot care should be performed with an interested and skilled farrier. Most of these cases show either poor hoof conformation or a hoof capsule distortion with prolapsed frogs or recessed frogs, long toe–low heel, or clubfoot conformation. Improving the foot conformation will redistribute the forces on the solar surface of the foot which in turn will decrease the stresses on the coronet. To accomplish the appropriate farriery, the author has found the best method is to remove the shoes initially and begin treatment in the barefoot state. If the frog is prolapsed below the hoof wall and there is a fissure in the central sulci of the frog, leaving the horse barefoot will reposition the frog to the same plane as the heels of the hoof capsule, the fissure will heal and the frog will no longer be traumatized. Otherwise, the heels of the hoof capsule are trimmed to where the frog and the hoof capsule are on the same plane and the rest of the hoof capsule is shaped as described in a recent paper on barefoot methodology.9 The horse is mildly sedated with the clinician’s medication of choice allowing the horse to remain coordinated. The hair around the entire coronary band is clipped using a number 40 surgical clipper blade. All loose exfoliating horn is removed from the frog with a sharp hoof knife. The affected hoof is placed on a farrier foot stand and the bulk of the abnormal hoof wall, crusts, and scales are removed with the smooth side of a farrier rasp. The same procedure is performed over the bulbs of the heels to the base of the frog. A medium-grit sanding block is then used to continue sanding the coronet and bulbs until there is a clear demarcation between the skin and the coronet. Following debridement, there may be some serous exudate or mild hemorrhage in which case a dry bandage can be placed for 24 hours. The horse is bedded with wood shavings or sawdust for the drying effect and turned out in a small dry paddock for a few hours per day if dry. The wear on the frog should not exceed new horn growth being produced, so it is important that the footing is not too hard, or shoes can be replaced if necessary. The coronary bands are cleaned every few days with a medium grit sanding block, then wiped with a moist gauze pad with saline and a thin layer of either a hydrocortisone 2.5% ointmenth or a betamethasone 0.5%/allantoin 1.5% ointmenti is applied. The frogs are cleaned daily with a wire brush and then painted with solution of benzoyl peroxide in 10% acetonej . This treatment is continued by the horse’s caretaker until the new growth has normalized and then as needed if symptoms begin to return (Fig. 5).
Canker Seven of the horses developed canker in various feet subsequent to showing signs of CBD. This may show a correlation between the two disease entities and CBD may predispose the foot to canker. The gross appearance of canker is generally diagnostic, but a biopsy is always an option for confirmation in these cases. The biopsy is generally read out as chronic proliferative pododermatitis.10 The coronary bands and the bulbs showing CBD were treated as described earlier in the text. Briefly, the treatment of canker consists of placing a tourniquet above the fetlock to provide a bloodless field which will enhance careful and thorough debridement of all disease tissue to where there is a clear demarcation between normal and abnormal tissue. The demarcation can be observed by a change in the appearance and consistency of the frog along with small pin-point hemorrhages noted in the tissue. Debridement is then followed by cryotherapy. Benzoyl peroxide in 10% acetone combined with metronidazole powder is applied to the debrided area and the foot is bandaged. The bandages are changed every second day, the debrided tissue is cleaned with a suitable mild antiseptic solution, rinsed with saline, and then the medication and bandages are reapplied.10 The use of shoes and treatment plates are discouraged as a dry environment on the solar surface of the foot is preferred. Once the frogs have healed and cornified, the treatment continues as outlined for CBD (Fig. 6). The treatment may seem involved but can be performed very efficiently by the horse’s caretaker on a daily or every-second-day basis in a short period of time.
Results All horses in this study responded to the described treatment protocol and returned to full work. Success was described as marked improvement in coronary band and hoof appearance within 3 to 6 weeks after treatment was initiated. In addition, horses returned to full work when shoes were replaced, horses had an acceptable macroscopic appearance of the coronary band and hoof wall, required minimal daily foot care, and were able to be reduced to at least every-other-day steroid administration and remain disease free (Fig. 7, A–C). Again, it must be emphasized, that due to the suspected genetic and auto-immune implications of this disease, permanent remission is generally not achieved. Discussion To the author’s knowledge, there are only two reports in the literature on CBD and one is a pathology report.3,4 These reports described the clinical signs and diagnosis but provided minimal information on treatment. This report details both systemic treatment as well as in-depth foot care as the combination appears to be necessary for improvement. As long-term corticosteroids are necessary for treatment, it strongly suggests CBD to be an immunemediated disease. These horses appear to have a specific antigen associated with the keratinized hoof wall that is involved. Pemphigus remains a possible cause as it has several subtypes that could affect an antigen located in a single type of tissue. A descending dose of prednisolone was chosen due to its good bioavailability, excellent anti-inflammatory effects and appears to be a minimal risk factor for developing laminitis.11 Minocycline, an oral antibiotic with good bioavailability and good tissue penetration, was used at the initiation of treatment for the possibility of a low-grade infection in the coronet. Foot care combined with the initial systemic therapy appears to be essential for a successful outcome. Taking the horse out of work during the initial treatment phase allows the feet to rest and prevents trauma to the healing tissue. Removing the shoes allows the feet to be trimmed properly, effectively improves any hoof capsule distortions or abnormal hoof conformation, and leaves all the affected tissue readily accessible for daily treatment. It appears important to remove all abnormal horn and crusts from the coronet and bulbs to allow penetration of the topical medication at the skin coronet junction. The topical corticosteroid ointment or the combination of betamethasone for its anti-inflammatory effect and allantoin for its astringent properties appear to be effective in decreasing abnormal growth. The affected tissue at the bulbs (and frogs) will generally be soft, void of adequate horn thickness, and contain multiple fissures. The use of benzoyl peroxide in 10% acetone as an astringent seems to improve the horn and promote cornification. If canker is present, the frog is treated as a separate entity as described above in combination with treatment for CBD. The final, essential, and extremely important aspect of this treatment is the commitment of the owner/caretaker to persevere through with the treatment plan. Although the treatment is not difficult; it is time consuming and the treatment not only has to be performed daily or on a frequent basis but must be thorough, consistent, and with attention to detail.
Acknowledgments
References and Footnotes
|