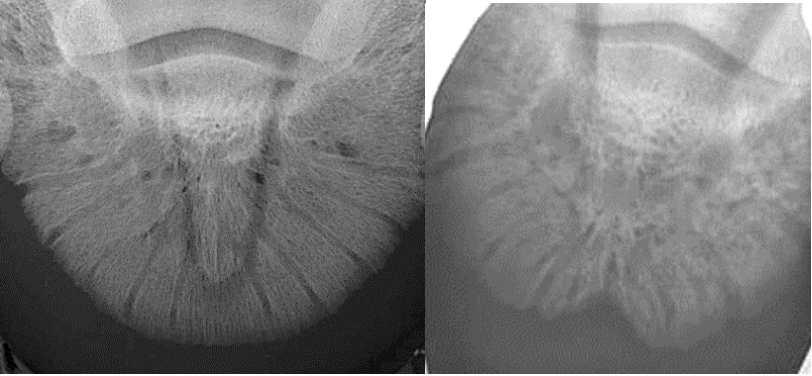
| Seedy Toe VS. White Line Disease Stephen E. O’Grady, DVM Being both a veterinarian and a farrier, I have had the opportunity to examine hundreds of feet that I had radiographed. There is often a notch in the distal dorsal border of the distal phalanx (DP) called the crena marginis solaris noted on a dorso-palmar radiograph. This is not an abnormal radiographic finding; however, the notch in the bone can vary in size and depth (Figure 1). It was always this author’s opinion that there was a correlation between a large or significant crena and a defect in the sole-wall junction or white line. The defect is directly dorsal to the crena and manifests as a cavitation in the sole-wall junction, often extending into the hoof wall leading to a small toe crack at the bearing border of the hoof wall. Recently, Travis Burns, CJF, FWCF from the Virginia Maryland Regional College of Veterinary Medicine submitted an excellent paper on this topic as his thesis for his FWCF certification. Although the study involved a limited number of horses, it confirmed a distinct correlation between the crena, and the clinical hoof wall defect known as seedy toe. Please see here.
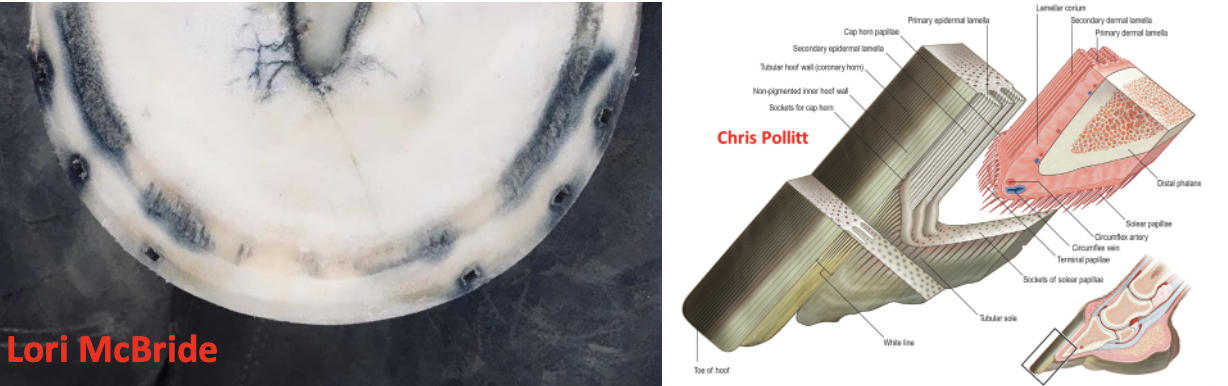
Seedy Toe Seedy toe is often characterized as white line disease (WLD) or a form of WLD which may not be accurate as they may be two different entities. The sole-wall junction (white line) is formed by the proliferation of basal cells from the keratinized epidermal lamellae along with tubular horn formed from the epidermis overlying the terminal papillae. The tubular horn fills the space between the inner layer of the hoof wall and the sole. The crena located in the bone disrupts the continuity of the dermis on the parietal surface of the DP to the distal border and the cavitation formed by the notch appears to interfere with the formation of the sole-wall junction. It can readily be seen from Burns’ study that this void will affect the interaction of the primary epidermal lamellae in forming the white line. It is also the author’s opinion there is a displacement of the circumflex circulation in this area but this needs to be substantiated with vascular studies (Figure 2). The size of the resultant defect at the sole-wall junction at the toe appears to be dependent on the size of the crena. Many of these defects become extensive and lead to a small vertical toe crack at the bearing border of the hoof wall (Figure 3). Interestingly, the dorsal, lateral, and medial boundaries of the defect also appear to be related to the size of the crena. Furthermore, when a resection is performed, the shape of the resection will mimic the size of the crena and length of the hoof wall at the toe (Figure 4). Farriery is important in addressing seedy toe and preventing its progression. Attention to foot conformation and trimming protocols is essential as increased leverage or increased load on the dorsal hoof wall will potentiate the defect. I see no reason to resect or invade these defects unless there is infection or an extensive toe crack. The presence of the crena will cause the defect to reappear as the resection grows out.
White Line Disease WLD lacks a definitive definition. However, WLD describes a keratinolytic process that originates on the solar surface of the hoof characterized by a progressive pathological separation of the inner zone of the hoof wall. The separation can extend to any area within the hoof capsule but never invades the coronet. Rather than expound on all the aspects of WLD here, the reader is urged to see here. There appears to be a stark difference between seedy toe and white line disease and perhaps they should not be grouped together in the same context. Seedy toe is a focal defect that affects the sole-wall junction while WLD is a diffuse defect that affects the inner part of the hoof wall. Be Safe. |